| x | x | |||||
|
|
 |
|||||
| INFECTIOUS DISEASE | BACTERIOLOGY | IMMUNOLOGY | MYCOLOGY | PARASITOLOGY | VIROLOGY | |
|
|
|
|||||
| SHQIP - ALBANIAN | ||||||
|
Let us know what you think FEEDBACK |
||||||
| SEARCH | ||||||
|
|
||||||
|
|
||||||
|
Logo image © Jeffrey Nelson, Rush University, Chicago, Illinois and The MicrobeLibrary |
||||||
|
|
||||||
|
All
life cycle diagrams in this section are courtesy of the
DPDx
Parasite Image Library
PART ONE |
Numerous species of arthropods play a role in human
disease. Most of these are as vectors of different pathogens and, in other
sections of this text, we have dealt with such disease vectors. There are also a number of arthropods
that cause harm due their venom but these are not parasites. Here, we shall deal
with arthropods that are parasitic to and cause disease in man. For
example, myiasis (burial of larvae in tissue) is an obligatory
step in the life cycle of some flies and incidental for others. Species that
cause myiasis in the Americas are Cochliomyia (Screw worm fly), Calliphora,
Oestrus, Sarcophaga, Gastrophilus, etc. Myiasis may be cutaneous, arterial,
intestinal or urinary in normal tissue or in pre-existing wounds, some of which
may result from other
infections. Larvae can burrow through necrotic or healthy tissue using their
mandibular hooks aided by proteolytic enzymes. They can cause mechanical
damage and the affected area may be the site of a secondary infection. Cutaneous myiasis may require surgical removal of burrowed larvae.
Eggs and maggots may be washed from hair, skin and wounds with soap and water.
Urinary myiasis usually clears itself. Purgation with anti-helminths may be
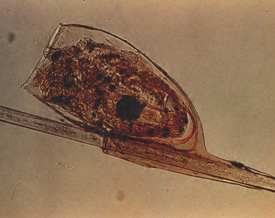
necessary for gastrointestinal myiasis. LICE Three types of sucking lice are important for human health: Pediculus humanus capitis (head louse), P. humanus humanus (body louse) and Pthirus pubis (crab louse). Lice spend all of their life on one very specific host and both male and female feed on blood and leave one host only to transfer to another (figure 1and 2).
|
|||||
|
WEB
RESOURCES |
||||||
|
|
 Figure 1
Figure 1 Life Cycle of the Head Louse The life cycle of
the head louse has three stages: egg, nymph, and adult.
|
|||||
|
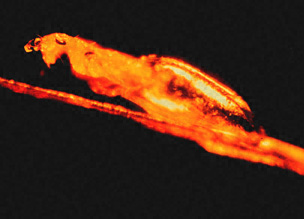
Figure 2
|
 C. Head Lice: Adult louse and two nymphs. The adult louse is about the size of a sesame seed, has 6 legs (each with claws), and is tan to grayish-white. In persons with dark hair, the adult louse will appear darker. Females lay up to 8 nits per day. Females are usually larger than males. CDC
|
|||||

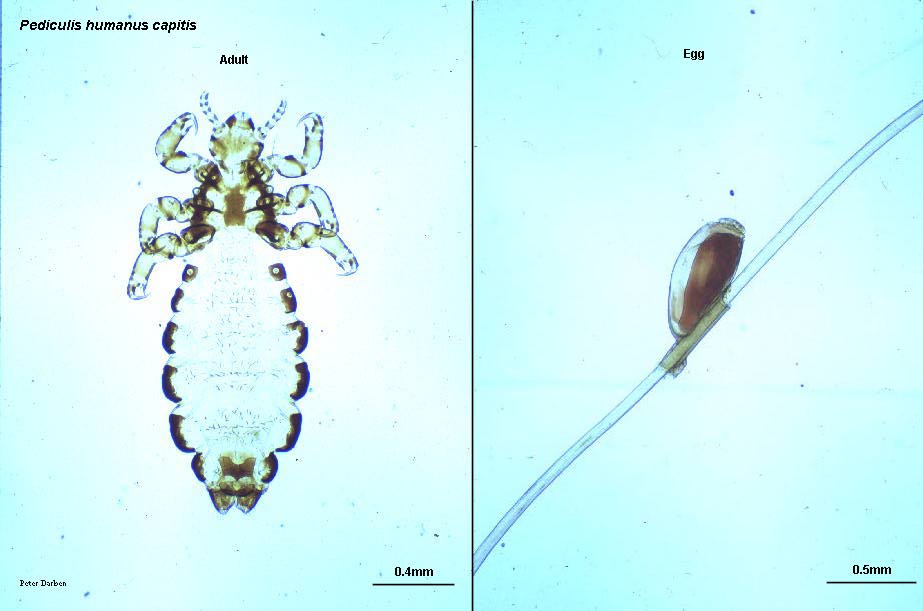
E. Female head louse, Pediculus humanus var capitis CDC/Dr. Dennis D. Juranek ddj1@cdc.gov 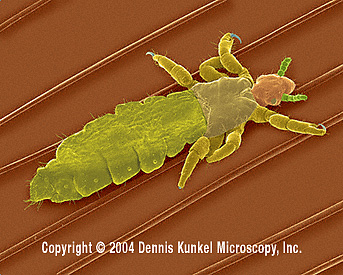
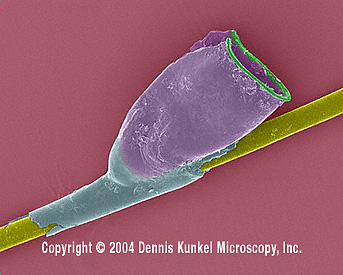
G. Head Louse on Human Hair - Pediculus humanus capitis (SEM x55) © Dennis Kunkel Microscopy, Inc. Used with permission
|
||||||
|
||||||
|
||||||
|
Figure 3 |
 D. Pubic Louse, Phthirus pubis adult © PeterDarben, used with
permission
D. Pubic Louse, Phthirus pubis adult © PeterDarben, used with
permission |
|||||
|
|
Most fleas (figure 4) are of clinical significance to man because they are vectors for other parasites. However, the jigger flea or chigoe (Tunga penetrans) is a serious pest in the tropical and subtropical regions of the Americas and Africa. Diagnosis of tungiasis is rare in North America. An epidemiological study in a traditional fishing village in Ceará State, north-eastern Brazil found about 51% of the population was infested Both sexes feed on blood. The female flea, after insemination, burrows itself in the skin of the toes and the sole of the foot. The female swells to the size of a pea, produces eggs and dies in the tissue. There is local reaction to the bite and the eggs and dead flea produce reaction. The infested tissue can get infected and gangrenous; auto-amputation is not uncommon. Treatments are symptomatic: infestation may be physically removed; secondary infections are treated appropriately. Shoes should be worn in infested areas.
|
|||||
|
Figure 4
|
 C. Tunga penetrans is known as the chigger, jigger, chigoe, bicho do pé or sand flea. The head is angular, it has no comb of spines, and the thoracic segments are narrow at the top.The female feeds by burrowing into the skin of its host. The abdomen becomes enormously enlarged between the second and third segments so that the flea forms a round sac with the shape and size of a pea © Marcelo de Campos Pereira, PhD, University of Sao Paulo. Used with permission
|
|||||
|
|
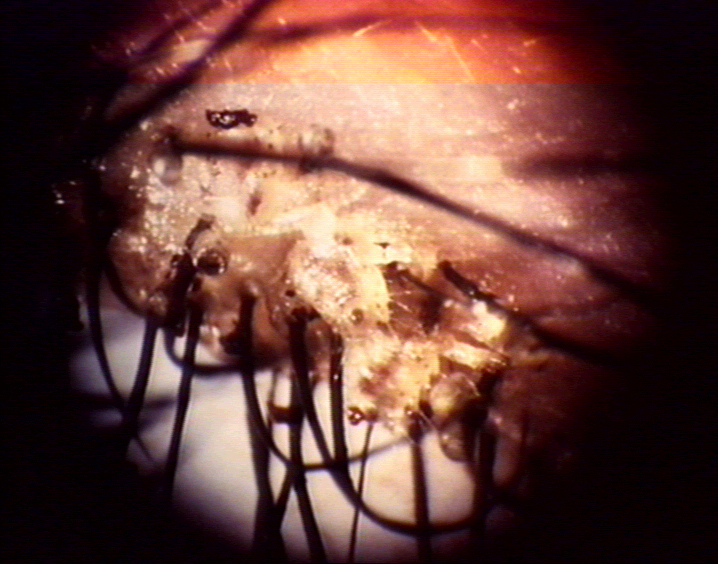
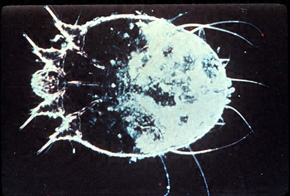
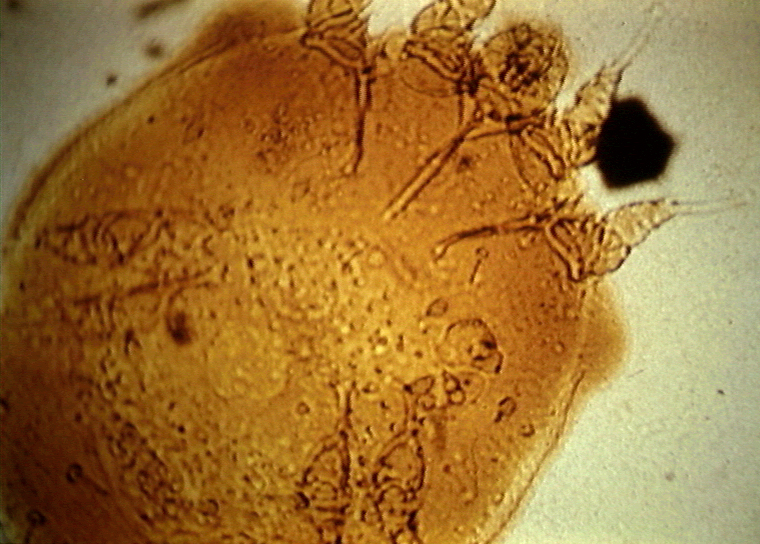
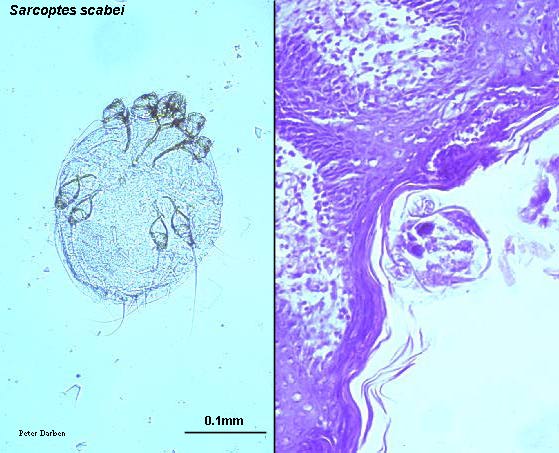
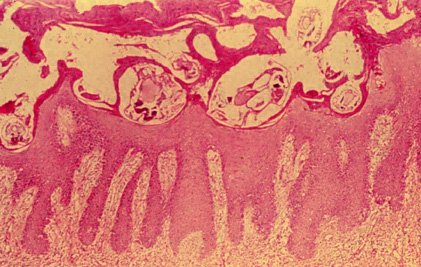
MITES Scabies mite (Sarcoptes scabei) (figure 5) is the cause of scabies and is distributed worldwide. Epidemics of the disease may occur for long periods but mites may be common at all times in very poor communities with inadequate washing facilities. The mite transmitted by contact burrows into the skin on the webbing side of fingers, later spreading to the wrists, elbows and the rest of the body (figure 6 and 7). The buttocks, women's breasts and external genitalia may be involved. The mite tunnels itself through the upper layer of the skin depositing eggs. Larvae escape the tunnel and wander on the skin and start new burrows and mature there to continue the cycle. Scabies itch is due to the sensitization of the patient to the mite and eggs and is characteristically nocturnal. Septic pustules may develop after scratching, if the hygiene is poor. Diagnosis is made by the characteristic rash and by smearing black ink on the skin and observing burrows when the ink is wiped away. Microscopic examination of a skin scraping shows the mites. Treatment involves swabbing of the whole body from the neck down with 1% malathion or benzene hexachloride (crotamiton for infants). Topical steroids must not be used. If possible, the whole family should be treated. Contact with an infested person should be avoided. Clothes should be washed in hot water.
|
|||||
|
Figure 5
|
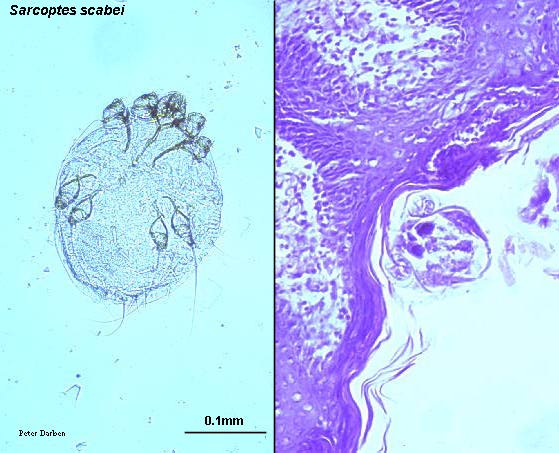 C.
Sarcoptes scabei adult, whole and in section of skin (H&E)
© PeterDarben, used with permission
C.
Sarcoptes scabei adult, whole and in section of skin (H&E)
© PeterDarben, used with permission |
|||||
|
Figure 6 |
Life cycle of the Scabies mite (Sarcoptes scabei) Sarcoptes scabei undergoes four stages in its life cycle; egg, larva, nymph and adult. Females deposit eggs at 2 to 3 day intervals as they burrow through the skin Transmission occurs by the transfer of ovigerous females during personal contact. Mode of transmission is primarily person to person contact, but transmission may also occur via fomites (e.g., bedding or clothing). Mites are found predominantly between the fingers and on the wrists. The mites hold onto the skin using suckers attached to the two most anterior pairs of legs. |
|||||
|
Figure 7
|
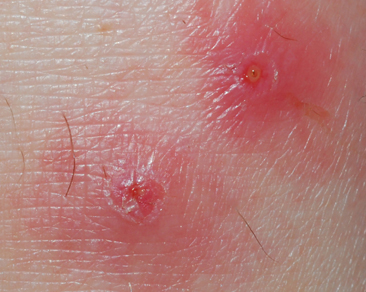
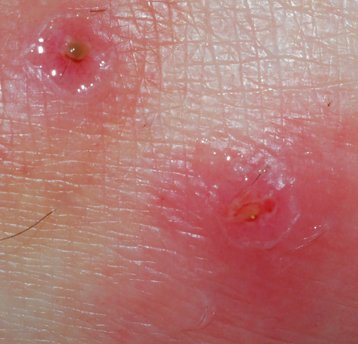
 C. Cross sectional view of the burrows created in the epithelium by Sarcoptes scabei.
CDC
C. Cross sectional view of the burrows created in the epithelium by Sarcoptes scabei.
CDC |
|||||
 Figure 8A
Figure 8A24hrs after a chigger bite, genus Trombicula, this patient presented with a red welt or bleb at the bite site. These chiggers can cause intense itching and reddish welts on skin, but are not known to transmit infectious diseases in the U.S. However, in some Asian countries, they are vectors of scrub typhus. CDC/M. A. Parsons  Figure 8B
Figure 8BChigger (adult) actual size 1/128 inch. Clemson University, South Carolina 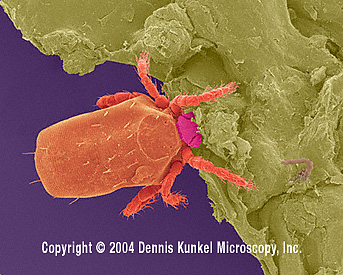 Figure
8C Figure
8CChigger mite © Dennis Kunkel Microscopy |
Chiggers (the larvae of red mites or harvest mites - figure 8) (Trombiculidae) are an important group of ectoparasites affecting humans. They attach to the skin in the ankles, waistline, armpits and perianal area after the host walks through a grassy environment. Contrary to popular belief, these mite larvae do not feed on blood and do not burrow into the skin. They pierce the skin near a hair follicle and feed on partially digested skin cells using enzymes in the chigger's saliva. They then drop off the host. The host reacts to the mouth parts and saliva of the mite, however, and after a few hours an erythematous papule appears (figure 8) that is highly pruritic. The intensity of the eruption depends on the sensitivity of the host and may be followed by fever. Treatment with a local anesthetic is useful. Insect repellents (DEET) may be effective in avoiding chigger bites. In south Asia, chiggers are the vectors for scrub typhus (Orientia tsutsugamushi), a rickettsial disease that can (rarely) be life-threatening. |
|||||
 Figure 9A.
Figure 9A.First instar larva of Cuterebra, The north American botfly which causes warbles in a variety of mammals but does not usually infect humans. CDC/Dr. George Healy
|
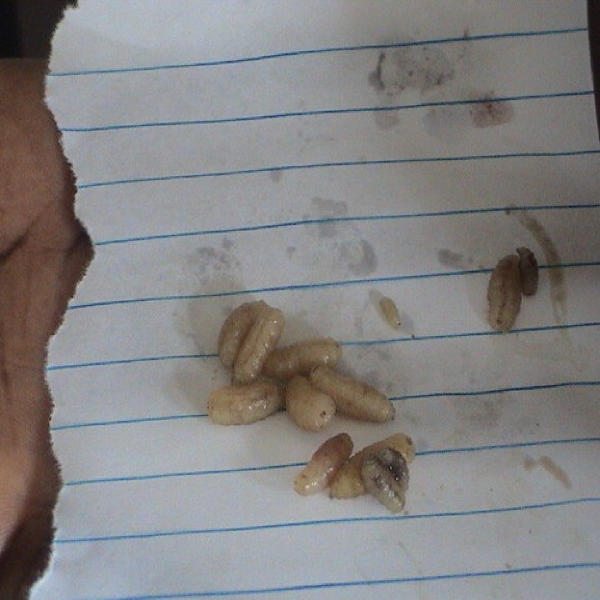
BOT FLY AND TUMBU FLY - Myiasis Myiasis is the parasitism of a vertebrate host by the larva of a dipteran fly. It frequently occurs in domestic and wild animals and therefore is important in veterinary medicine. Human cases are rare but occur especially in tropical countries. In the United States, the most common agents of myiasis are Dermatobia hominis (bot fly, berne) and Cordylobia anthropophaga (tumbu fly). The former occurs in central (particularly Mexico and Belize) and south America and some Caribbean islands such as Trinidad, while the latter occurs in tropical Africa. The larvae of both of these flies are obligate parasites of mammals. The human bot fly has a very interesting life cycle. The female fly captures a mosquito and lays its eggs on its abdomen. When the released mosquito takes a blood meal (usually on the face, scalp or extremities), the body heat of the mammal causes the eggs to hatch into a first instar larva, which drops onto the skin of its host. The larva either enters the skin via the puncture wound made by the mosquito or actively penetrates the skin where it takes up residence in sub-cutaneous tissue. Here, the larva matures through second and third instars over a period of one or two months. The larvae are difficult to remove because of backward facing barbs (figure 9). When they are mature, the larvae emerge and fall to the ground where they pupate into the adult fly and the life cycle repeats. The adult fly only lives a few days and does not feed. The initial symptom of the presence of a bot fly is a cutaneous nodule that contains one larva (although this is not initially visible). The nodule is often called a warble or a furuncle and myiasis is often referred to as a furunculous disease. Unlike a puncture wound of a mosquito, the infected nodule discharges blood or serum continually because the larva needs to keep the wound open in order to breath. There is often pruritus and sometimes intense periodic shooting pain that occurs when the larva moves or matures to another instar. As the larva grows, movement can often be seen below the surface of the serosanguineous effusion. There may also be local lymphadenopathy, and fever and malaise if a secondary bacterial infection develops. Treatment entails removal of the larva, although some patients prefer to allow the larva to develop and emerge naturally. In the case of Dermatobia hominis, the Achilles heel is the need for the larva to breath air through the open wound. Cutting off the parasite's air supply is most often done by applying a thick layer (at least 5mm) of Vaseline, although nail polish, adhesive tape and even bacon have been reported to be used. Because of the lack of oxygen, the larva will usually emerge and can be pulled the remaining way out with forceps. However, it often takes a day for the larva to come far enough out to be grabbed with forceps. Surgery is not usually necessary unless the larva dies in situ and cannot be removed. Tumbu fly (Cordylobia anthropophaga) is found in sub-Saharan Africa and causes a furuncular myiasis similar to bot fly (figure 10). The patient comes in contact with eggs on the ground or deposited on clothes. After hatching, the larva burrows into the skin. The eggs are killed by ironing clothes but for many people that may be impractical.
|
|||||
|
VIDEO |
||||||
 Figure 9 E
Figure 9 E Dermatobia hominis (Bot fly) Frontal view. Bot fly is a bluebottle-like fly with yellow to orange head and legs. The thorax is dark blue with a greyish bloom; the abdomen is short and broad and has a brilliant blue color. Adults have atrophied mouthparts and do not feed, relying instead on food reserves accumulated during the larval stage. © Marcelo de Campos Pereira, PhD, University of Sao Paulo. Used with permission  Figure 9F
Figure 9F Dermatobia hominis Female lateral view © Marcelo de Campos Pereira, PhD, University of Sao Paulo. Used with permission  Figure 9G
Figure 9G Eggs of Dermatobia hominis Eggs are glued to the abdomen of a carrier fly. When the Dermatobia female is ready to oviposit, she captures another insect - usually a fly - and glues her eggs to the captured insect's abdomen. © Marcelo de Campos Pereira, PhD, University of Sao Paulo. Used with permission
|
||||||
|
CASE REPORT |
||||||
|
VIDEO |
||||||
|
|
||||||