|
x |
x |
|
 |
 |
|
INFECTIOUS
DISEASE |
BACTERIOLOGY |
IMMUNOLOGY |
MYCOLOGY |
PARASITOLOGY |
VIROLOGY |
|
|
PARASITOLOGY - CHAPTER SIX
TREMATODES (FLUKES)
Dr Abdul Ghaffar
Professor Emeritus
University of South Carolina School of Medicine
|
|
|
|
SHQIP - ALBANIAN |
|
|
Let us know what you think
FEEDBACK |
|
SEARCH |
|
|

 |
|
Logo image © Jeffrey
Nelson, Rush University, Chicago, Illinois and
The MicrobeLibrary |
|
All
life cycle diagrams in this section are courtesy of the
DPDx
Parasite Image Library
Centers for Disease Control (CDC) |
|
TEACHING OBJECTIVES
Epidemiology,
morbidity and mortality
Morphology
of the organism
Life
cycle, hosts and vectors
Disease,
symptoms, pathogenesis and site
Diagnosis
Treatment,
prevention and control |
The most significant trematodes from a
clinical point of view are blood flukes, Schistosoma mansoni, S. japonicum and
S. hematobium. Other trematodes of significance are intestinal fluke,
Fasciolopsis buski, liver fluke, Clonorchis sinensis and lung fluke,
Paragonimus westermani.
Schistosomiasis (Bilharziasis)
The three species of Schistosoma have
different geographic distributions. S. hematobium is prevalent in Africa,
S.
mansoni is found in Africa and America and S. japonicum is common in the far
east.
Epidemiology
Approximately 250
million people are infected with schistosomes and 600 million are at risk.
Morphology
Adult worms are 10 to 20 mm long; the male has an unusual lamelliform shape with marginal folds
forming a canal in which the slender female worm resides. Unlike other
trematodes, schistosomes have separate sexes (figure 1).
Life cycle
Man is infected by
cercaria in fresh water by skin penetration. The cercaria travel through the venous
circulation to the heart, lungs and portal circulation. In about 3 weeks, they
mature and reach the mesenteric (S. japonicum and S. mansoni) or the bladder
(S. hematobium) vessels where they live and ovulate for the duration of
the host's life.
Eggs germinate as they pass through the vessel wall into the intestine or bladder
and are excreted in feces (S. japonicum and S. mansoni) or urine
(S. hematobium).
In fresh water, the larval miracidium hatches out of the egg and swims about
until it finds an appropriate snail. After two generations of multiplication in
the snail, the fork-tailed cercariae emerge into the water and infect another human
(figure 2).
Symptoms
Penetration of
cercariae causes transient dermatitis (swimmers' itch). The symptoms of
schistosomiasis are primarily due to a reaction against the eggs and include
splenomegaly, lymphadenopathy and diarrhea. In the bladder, they produce
granulomatous lesions, hematuria and sometimes urethral occlusion. Most bladder
cancers in endemic areas are associated with chronic infection. In the
intestine, they cause polyp formation which, in severe cases, may result in life
threatening dysentery. In the liver, the eggs cause periportal fibrosis and
portal hypertension resulting in hepatomegaly, splenomegaly and ascites. A gross
enlargement of the esophageal and gastric veins may result in their rupture. S.
japonicum eggs are sometimes carried to the central nervous system and cause headache,
disorientation, amnesia and coma. Eggs carried to the heart produce
arteriolitis and fibrosis resulting in enlargement and failure of the right
ventricle (figure 2a).
Pathology and Immunology
The
'swimmers' itch is due to physical damage to the skin by proteases and other
toxic substances secreted by the cercaria. The host develops both type I and
type IV hypersensitivity reactions to schistomal secretions and egg
constituents. Embryonated eggs cause collagenase-mediated damage to the vascular
endothelium. Host immune responses, both humoral and cell mediated, have been
shown to be of some protective value. IgE and eosinophil mediated cytotoxicity
has been suggested as a mechanism of killing the adult worm.
Diagnosis
Diagnosis is
based on a history of residence in an endemic area, swimmers' itch and other
symptoms. The eggs are very characteristic and confirm diagnosis. S.
hematobium eggs in urine (55 to 65 by 110 to 170 micrometers) have an apical spine or
knob. S. mansoni eggs in feces (45 to 70 by 115-175
micrometers) have a spine
on the side. S. japonicum eggs (55 to 65 by 70 to 100 micrometers) are more round
with a vague spine
on the side.
Treatment and control
Praziquantel is effective against all species. Contaminated water should be
avoided. Control measures include sanitary disposal of sewage and destruction of
snails. No vaccine is available.
|
|
|
|
|

 Figure 1A
Figure 1A
Schistosomes. WHO
 Figure 1B
Figure 1B
Male and female
schistosomes. (Drawn by Sylvia Treadgold) WHO
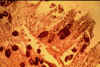 Figure 1C
Figure 1C
Intestinal
schistosomiasis: eggs in the wall of the gut.
WHO
 Figure 1D
Figure 1D
Schistosoma haematobium egg ©
Dr Peter
Darben, Queensland University of Technology clinical parasitology
collection. Used with permission

 Figure 1E
Figure 1E
Eggs of Schistosoma haematobium (A). In this species, the eggs are large and have a
prominent terminal spine at the posterior end.
Length 112-170 µm. In (B), a greater magnification shows the miracidium inside the egg.
CDC
 Figure 1F
Figure 1F
Schistosoma haematobium adult male ©
Dr Peter
Darben, Queensland University of Technology clinical parasitology
collection. Used with permission
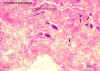 Figure 1G
Figure 1G
Schistosoma haematobium eggs in section of bladder (H&E) ©
Dr Peter
Darben, Queensland University of Technology clinical parasitology
collection. Used with permission
 Figure 1H
Figure 1H
Schistosoma japonicum adult male and female, in copula ©
Dr Peter
Darben, Queensland University of Technology clinical parasitology
collection. Used with permission
A
 B
B
 Figure 1I
Figure 1I
Egg of Schistosoma japonicum (A). The egg is typically oval or
subspherical, and has a vestigial spine, which is better shown in
(B). Schistosoma japonicum eggs are smaller (68 - 100 µm by 45 - 80 µm) than those of the other species.
CDC
 Figure 1J
Figure 1J
Schistosoma japonicum egg ©
Dr Peter
Darben, Queensland University of Technology clinical parasitology
collection. Used with permission
 Figure 1K
Figure 1K
Schistosoma japonicum adult male and female ©
Dr Peter
Darben, Queensland University of Technology clinical parasitology
collection. Used with permission
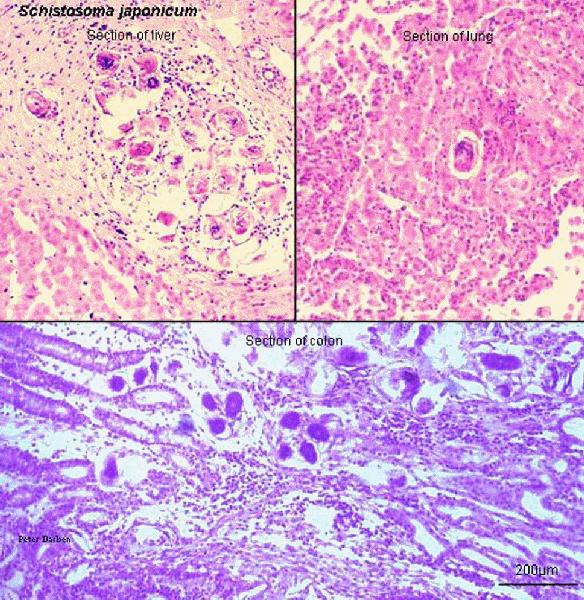
 Figure 1L
Figure 1L
Schistosoma japonicum eggs in tissue section (H&E) ©
Dr Peter
Darben, Queensland University of Technology clinical parasitology
collection. Used with permission
A
 B
B
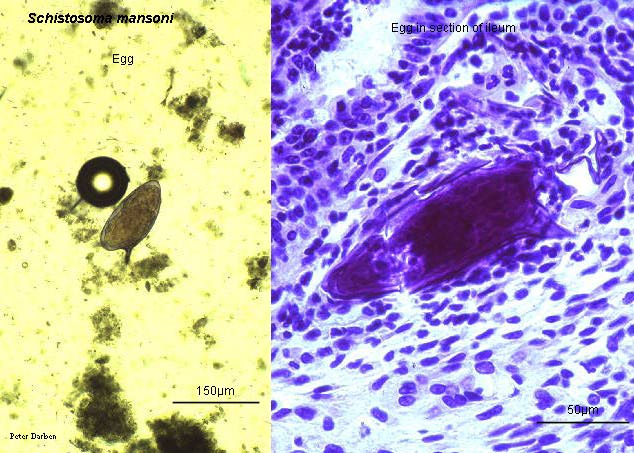
 Figure 1M
Figure 1M
Eggs of Schistosoma mansoni in a patient from Egypt. These eggs are large (length 114 - 180 µm) and have a characteristic shape, with a prominent lateral spine near the posterior end. The anterior end is tapered and slightly curved. When the eggs are excreted, they contain a mature miracidium (visible especially in A).
CDC
 Figure 1N
Figure 1N
Schistosoma mansoni adult male and female ©
Dr Peter
Darben, Queensland University of Technology clinical parasitology
collection. Used with permission
 Figure 1O
Figure 1O
Schistosoma mansoni adult male and female, in copulo ©
Dr Peter
Darben, Queensland University of Technology clinical parasitology
collection. Used with permission
 Figure 1P
Figure 1P
Schistosoma mansoni egg, whole and in section (H&E) ©
Dr Peter
Darben, Queensland University of Technology clinical parasitology
collection. Used with permission
 Figure 1Q
Figure 1Q
Schistosoma mansoni miracidium ©
Dr Peter
Darben, Queensland University of Technology clinical parasitology
collection. Used with permission
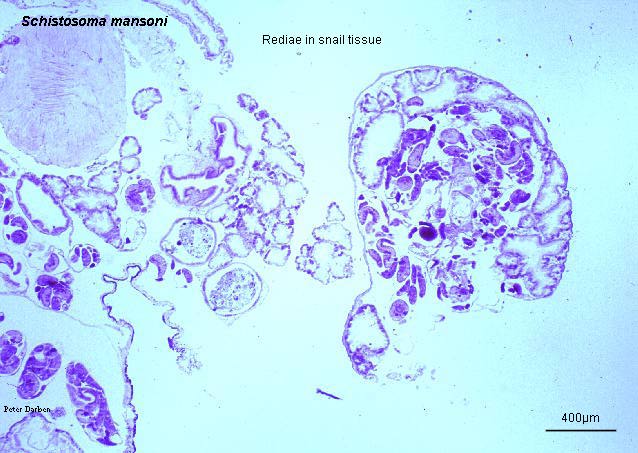
 Figure 1R
Figure 1R
Schistosoma mansoni in section of snail tissue (H&E) ©
Dr Peter
Darben, Queensland University of Technology clinical parasitology
collection. Used with permission
 Figure 1S
Figure 1S
Schistosoma mansoni cercaria ©
Dr Peter
Darben, Queensland University of Technology clinical parasitology
collection. Used with permission |
| |
| |
| |
| |
|
|
 Figure 1T
Figure 1T
Life cycle of schistosomes
Eggs are
eliminated with feces or urine
 .
Under optimal conditions the eggs hatch and release miracidia .
Under optimal conditions the eggs hatch and release miracidia
 ,
which swim and penetrate specific snail intermediate hosts ,
which swim and penetrate specific snail intermediate hosts
 .
The stages in the snail include 2 generations of sporocysts .
The stages in the snail include 2 generations of sporocysts
 and the production of cercariae
and the production of cercariae
 .
Upon release from the snail, the infective cercariae swim, penetrate the
skin of the human host .
Upon release from the snail, the infective cercariae swim, penetrate the
skin of the human host  , and
shed their forked tail, becoming schistosomulae , and
shed their forked tail, becoming schistosomulae
 .
The schistosomulae migrate through several tissues and stages to their
residence in the veins ( .
The schistosomulae migrate through several tissues and stages to their
residence in the veins ( , ,
 ).
Adult worms in humans reside in the mesenteric venules in various
locations, which at times seem to be specific for each species ).
Adult worms in humans reside in the mesenteric venules in various
locations, which at times seem to be specific for each species
 .
For instance, S. japonicum is more frequently found in the
superior mesenteric veins draining the small intestine .
For instance, S. japonicum is more frequently found in the
superior mesenteric veins draining the small intestine
 ,
and S. mansoni occurs more often in the superior mesenteric veins
draining the large intestine ,
and S. mansoni occurs more often in the superior mesenteric veins
draining the large intestine
 .
However, both species can occupy either location, and they are capable
of moving between sites, so it is not possible to state unequivocally
that one species only occurs in one location. S. haematobium
most often occurs in the venous plexus of bladder .
However, both species can occupy either location, and they are capable
of moving between sites, so it is not possible to state unequivocally
that one species only occurs in one location. S. haematobium
most often occurs in the venous plexus of bladder
 ,
but it can also be found in the rectal venules. The females (size
7 to 20 mm; males slightly smaller) deposit eggs in the small venules of
the portal and perivesical systems. The eggs are moved
progressively toward the lumen of the intestine (S. mansoni and S.
japonicum) and of the bladder and ureters (S. haematobium),
and are eliminated with feces or urine, respectively
. Pathology
of S. mansoni and S. japonicum schistosomiasis includes:
Katayama fever, presinusoidal egg granulomas, Symmers’ pipe stem
periportal fibrosis, portal hypertension, and occasional embolic egg
granulomas in brain or spinal cord. Pathology of S. haematobium
schistosomiasis includes: hematuria, scarring, calcification, squamous
cell carcinoma, and occasional embolic egg granulomas in brain or spinal
cord. ,
but it can also be found in the rectal venules. The females (size
7 to 20 mm; males slightly smaller) deposit eggs in the small venules of
the portal and perivesical systems. The eggs are moved
progressively toward the lumen of the intestine (S. mansoni and S.
japonicum) and of the bladder and ureters (S. haematobium),
and are eliminated with feces or urine, respectively
. Pathology
of S. mansoni and S. japonicum schistosomiasis includes:
Katayama fever, presinusoidal egg granulomas, Symmers’ pipe stem
periportal fibrosis, portal hypertension, and occasional embolic egg
granulomas in brain or spinal cord. Pathology of S. haematobium
schistosomiasis includes: hematuria, scarring, calcification, squamous
cell carcinoma, and occasional embolic egg granulomas in brain or spinal
cord.
Human contact with
water is thus necessary for infection by schistosomes. Various
animals, such as dogs, cats, rodents, pigs, hourse and goats, serve as
reservoirs for S. japonicum, and dogs for S. mekongi.
|
|
|
 Figure 2A
Figure 2A
The abdomen of an 11-year-old boy with intestinal schistosomiasis with the size and extent of the liver and spleen marked. Both are well below the midline, indicating the severity of infection. The disease has caused a stunting of the boy's growth, he is only 120cms tall and weighs 22 kg.
WHO/TDR/Crump
 Figure 2B
Figure 2B
Two boys, victims of
schistosomiasis showing typical distension of the abdomen.
WHO
 Figure 2C
Figure 2C
A 13-year-old boy with schistosomiasis (bilharziasis).
Hepatosplenomegaly, ascites, muscle atrophy, pyrexia, anaemia and haemorrhage from the gastrointestinal tract.
WHO/TDR/Vogel |
| |
Fasciolopsis buski (Giant intestinal fluke)
Epidemiology
This is a
parasite of central and southeast Asia.
Morphology
The elongate
oval fluke is 2 to 7 cm long and lives in the small intestine of man (figure 3).
Life cycle
Man is infected
by ingesting water chestnuts contaminated with metacercaria which find access to
the small intestine, attach themselves to the mucosa and mature in 25 to 30 days.
The fluke eggs are passed in the feces and hatch in fresh water producing
miracidia which must penetrate a suitable snail within hours. The miracidia in
the snail develop into cercaria and enter fresh water where they attach
themselves
to water plants (water chestnut) and encyst to become metacercaria (figure 4).
Symptoms
Epigastric pain,
nausea and diarrhea are experienced, especially in the morning. In heavier
infections, generalized edema and ascites occur.
Pathology
The fluke
attaches itself to the intestinal mucosa where inflammation, ulceration and abscesses
occur.
Diagnosis
Diagnosis is
based on clinical symptoms in endemic areas. Eggs in feces (75 to 100 by 130 to
150 micrometers) provide the final diagnosis.
Treatment and control
Praziquantel has proven effective. Water chestnuts from contaminated
waters should be avoided. Sewage should be treated before disposal.
|
|
|
 Figure 3A
Figure 3A
Liver fluke, a trematode liver parasite - helminth (Fasciola spp.)
Mouth and pharynx of the adult liver fluke. Humans are infected by
ingestion of uncooked aquatic vegetation on which the metacercariae stage
is encysted. Metacercariae excyst in the duodenum and migrate through the
intestinal wall in to the peritoneal cavity. The larvae enter the liver by
penetrating the capsule and wander through the liver parenchyma for up to
9 weeks. Most damage is done in the liver parenchyma by physical
irritation and metabolic by products.
©
Dennis Kunkel Microscopy, Inc.
Used with permission
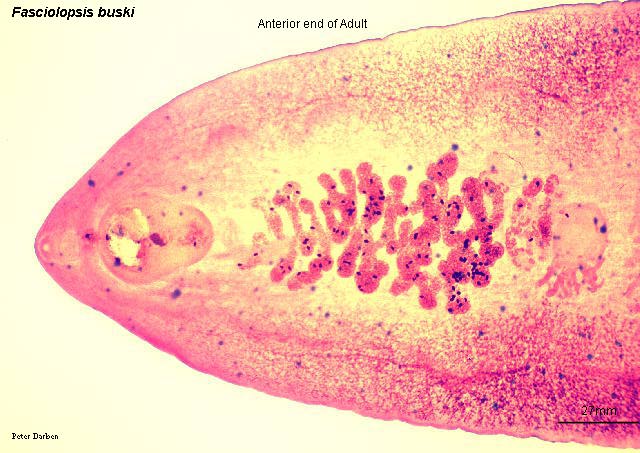
 Figure 3B
Figure 3B
Fasciolopsis buski adult, carmine stain © Dr
Peter Darben, Queensland University of Technology clinical
parasitology collection. Used with permission
 Figure 3C
Figure 3C
Fasciolopsis buski egg © Dr
Peter Darben, Queensland University of Technology clinical
parasitology collection. Used with permission |
|
|
 Figure
4 Figure
4
Life cycle of Fasciolopsis buski
Immature eggs are discharged into the intestine and stool
. Eggs become
embryonated in water , eggs
release miracidia , which
invade a suitable snail intermediate host
.
In the snail the parasites undergo several developmental stages (sporocysts
 , rediae , rediae
 ,
and cercariae ,
and cercariae  ). The
cercariae are released from the snail
and encyst as metacercariae on aquatic plants ). The
cercariae are released from the snail
and encyst as metacercariae on aquatic plants
 .
The mammalian hosts become infected by ingesting metacercariae on the
aquatic plants. After ingestion, the metacercariae excyst in the
duodenum .
The mammalian hosts become infected by ingesting metacercariae on the
aquatic plants. After ingestion, the metacercariae excyst in the
duodenum  and attach
to the intestinal wall. There they develop into adult flukes (20
to 75 mm by 8 to 20 mm) in approximately 3 months, attached to the
intestinal wall of the mammalian hosts (humans and pigs) and attach
to the intestinal wall. There they develop into adult flukes (20
to 75 mm by 8 to 20 mm) in approximately 3 months, attached to the
intestinal wall of the mammalian hosts (humans and pigs)
 .
The adults have a life span of about one year. .
The adults have a life span of about one year.
|
| |
Liver Flukes
Epidemiology Fasciola
hepatica, Opisthorchis (previously named Chlonorchis) sinensis,
O. felineus and O. viverini affect humans in various parts of the
world. F. hepatica is distributed worldwide and is a parasite of grazing
animals (sheep and cattle) and man. O. sinensis is a widespread parasite
of man, dogs and cats in southeast Asia. It is extraordinarily common in China
and is also found in Korea and Japan. Related Opisthorchis species
parasitizing European cats (Opisthorchis felinus) and SE Asian dogs (O.
viverini) infect humans in the endemic areas. Liver fluke cases are rare in
the United States, although snails harboring F. hepatica are present in
the western and southern parts of the US.
Fasciola hepatica
Morphology
F hepatica is leaf shaped and measures approximately 1 x 3 cm. The eggs
measure 80 x 150 µm.
Life cycle
Humans are infected by the consumption of improperly cooked watercress that
harbors encysted larval metacercariae. The larval fluke penetrates the duodenal
wall and migrates to the peritoneal cavity, penetrates the liver capsule and
migrates into the bile duct where it matures. The adult fluke passes its eggs in
stool that hatch in water to produce miracidia. The miracidium must find an
appropriate snail to continue the life cycle. In the snail, the miracidium
divides and gives rise to cercariae which exit the snail and encyst as
metacercariae attached to watercress leaves.
Symptoms
Passage of the larva through the liver produces tenderness and hepatomegaly. The
infection results in upper quadrant pain, chills and fever accompanied with
eosinophilia. The toxic secretions cause hepatitis. The presence of the worm in
the bile duct causes irritation resulting in hyperplasia of the epithelium and
bile obstruction. Adult worms may invade the liver and cause necrotic foci
(liver rot).
Diagnosis
Diagnosis is based on symptoms and history. The eggs in the stool are
indistinguishable from those of F. buski.
Treatment
In contrast with
F. buski, F. hepatica is not responsive to
praziquantel. However, Triclabendazole is effective.
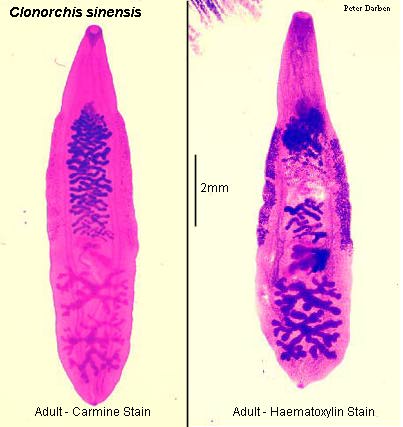
Opisthorchis sinensis, O.
felineus and O. viverini
Morphology
These are spindloid flukes measuring about 16x4 mm. The eggs measure 29 x 16 µm.
Life cycle
Man is infected by eating raw or improperly cooked fish that carries the
infective metacercaria in a cyst. The cyst is digested and the larval worm
migrates up the bile duct to liver where it matures into an adult. The eggs
deposited in the biliary duct pass in the feces and find their way to fresh
water. Upon ingestion by a suitable fresh water operculate snail, the egg
hatches to produce a miracidium. The miracidium in the snail develops into
cercaria that break out in water to penetrate under scales of fish. In fish, the
cercaria encysts in the muscle and forms the metacercaria that are infectious to
man.
Symptoms
The worm causes irritation of the bile ducts that become dilated and deviated.
The liver may become enlarged (hepatomegaly), necrotic and tender and liver
function may be impaired. Modest infections result in indigestion, epigastric
discomfort, weakness and loss of weight. Heavier infections produce anemia,
hepatomegaly, slight jaundice, edema, ascites and diarrhea.
Diagnosis
Diagnosis is based on symptoms and presence of endemic infection in the area.
Definitive diagnosis is dependent on finding the characteristic eggs in the
feces or biliary drainage.
Treatment and control
Praziquantel has proven to be of value. Fish should be cooked well before
consumption. Sewage must be treated before disposal.
|
|
|
 Figure 5A
Figure 5A
Clonorchis sinensis egg ©
Dr Peter
Darben, Queensland University of Technology clinical parasitology
collection. Used with permission
 Figure 5B
Figure 5B
Clonorchis sinensis adult, carmine and haematoxylin stain ©
Dr Peter
Darben, Queensland University of Technology clinical parasitology
collection. Used with permission
 Figure 5C
Figure 5C
Clonorchis sinensis adults in section of liver (H&E) ©
Dr Peter
Darben, Queensland University of Technology clinical parasitology
collection. Used with permission
|
|
|
 Figure 6
Figure 6
Embryonated
eggs are discharged in the biliary ducts and in the stool
.
Eggs are ingested by a suitable snail intermediate host
;
there are more than 100 species of snails that can serve as intermediate
hosts. Each egg releases a miracidia
 ,
which go through several developmental stages (sporocysts ,
which go through several developmental stages (sporocysts
 ,
rediae ,
rediae  , and cercariae , and cercariae
 ).
The cercariae are released from the snail and after a short period of
free-swimming time in water, they come in contact and penetrate the
flesh of freshwater fish, where they encyst as metacercariae
.
Infection of humans occurs by ingestion of undercooked, salted, pickled,
or smoked freshwater fish .
After ingestion, the metacercariae excyst in the duodenum ).
The cercariae are released from the snail and after a short period of
free-swimming time in water, they come in contact and penetrate the
flesh of freshwater fish, where they encyst as metacercariae
.
Infection of humans occurs by ingestion of undercooked, salted, pickled,
or smoked freshwater fish .
After ingestion, the metacercariae excyst in the duodenum
 and ascend the biliary tract through the ampulla of Vater
and ascend the biliary tract through the ampulla of Vater
 .
Maturation takes approximately 1 month. The adult flukes
(measuring 10 to 25 mm by 3 to 5 mm) reside in small and medium sized
biliary ducts. In addition to humans, carnivorous animals can
serve as reservoir hosts. .
Maturation takes approximately 1 month. The adult flukes
(measuring 10 to 25 mm by 3 to 5 mm) reside in small and medium sized
biliary ducts. In addition to humans, carnivorous animals can
serve as reservoir hosts.
|
| |
Paragonimus westermani
(Lung Fluke)
Epidemiology
Lung fluke is
most commonly encountered in parts of Asia, Africa and South America.
Morphology
It is a plump
reddish brown oval worm measuring 10 by 4 mm. The ovum measures 85 by 55 micrometers
(figure 7).
Life cycle
Lung fluke infects man
(and domestic carnivores) when crabmeat infested with encysted metacercaria is
consumed. The metacercaria reach the small intestine, exit their shell and bore
their way, as young flukes, through the intestinal wall, through the thoracic
diaphragm and penetrate the lung. There, they become enclosed in 1 to 2 cm cysts and
reach maturity. The eggs are found in the sputum or, if swallowed, in the feces,
2 to 3 months after infection. The eggs, when introduced in fresh water produce a
miracidia which penetrates the suitable snail. In the snail they develop into
cercaria which break out in water and penetrate gills, muscle or viscera of
fresh water crabs and become encysted in flesh as metacercaria (figure 8).
Symptoms
The fluke provokes
the development of a fibrous tissue capsule with bloody purulent material
containing eggs. There is inflammatory infiltrate around the capsule. The
symptoms include a dry cough, followed by production of blood stained rusty
brown sputum. Pulmonary pain and pleurisy may develop. Worms may migrate to the
brain where they lay eggs and cause a granulomatous abscess resulting in symptoms
similar to epilepsy.
Diagnosis
Diagnosis is
based on history and symptoms. Eggs are found in rust colored sputum, often
being examined for tuberculosis.
Treatment and control
Praziquantel
taken orally is quite effective. Adequate cooking of crustaceans is a preventive
measure. Improved sanitary conditions have lowered the infection rate in endemic
areas.
|
|
|
 Figure 7A
Figure 7A
Paragonimus westermani egg ©
Dr Peter
Darben, Queensland University of Technology clinical parasitology
collection. Used with permission
 Figure 7B
Figure 7B
Paragonimus westermani adult, carmine stain ©
Dr Peter
Darben, Queensland University of Technology clinical parasitology
collection. Used with permission
 Figure 7C
Figure 7C
Paragonimus westermani adult in section of lung (H&E)
©
Dr Peter
Darben, Queensland University of Technology clinical parasitology
collection. Used with permission |
|
|
 Figure 8
Figure 8
Paragonimus westermani (Lung Fluke) Life Cycle
The eggs are excreted unembryonated in the sputum, or
alternately they are swallowed and passed with stool
 .
In the external environment, the eggs become embryonated
,
and miracidia hatch and seek the first intermediate host, a snail, and
penetrate its soft tissues .
Miracidia go through several developmental stages inside the snail
:
sporocysts , rediae
,
with the latter giving rise to many cercariae
,
which emerge from the snail. The cercariae invade the second
intermediate host, a crustacean such as a crab or crayfish, where they
encyst and become metacercariae. This is the infective stage for
the mammalian host .
Human infection with P. westermani occurs by eating inadequately
cooked or pickled crab or crayfish that harbor metacercariae of the
parasite . The
metacercariae excyst in the duodenum
,
penetrate through the intestinal wall into the peritoneal cavity, then
through the abdominal wall and diaphragm into the lungs, where they
become encapsulated and develop into adults .
In the external environment, the eggs become embryonated
,
and miracidia hatch and seek the first intermediate host, a snail, and
penetrate its soft tissues .
Miracidia go through several developmental stages inside the snail
:
sporocysts , rediae
,
with the latter giving rise to many cercariae
,
which emerge from the snail. The cercariae invade the second
intermediate host, a crustacean such as a crab or crayfish, where they
encyst and become metacercariae. This is the infective stage for
the mammalian host .
Human infection with P. westermani occurs by eating inadequately
cooked or pickled crab or crayfish that harbor metacercariae of the
parasite . The
metacercariae excyst in the duodenum
,
penetrate through the intestinal wall into the peritoneal cavity, then
through the abdominal wall and diaphragm into the lungs, where they
become encapsulated and develop into adults
 (7.5 to 12 mm by 4 to 6 mm). The worms can also reach other organs
and tissues, such as the brain and striated muscles, respectively.
However, when this takes place completion of the life cycles is not
achieved, because the eggs laid cannot exit these sites. Time from
infection to oviposition is 65 to 90 days. Infections may persist for 20 years in humans. Animals such as pigs,
dogs, and a variety of feline species can also harbor P. westermani.
(7.5 to 12 mm by 4 to 6 mm). The worms can also reach other organs
and tissues, such as the brain and striated muscles, respectively.
However, when this takes place completion of the life cycles is not
achieved, because the eggs laid cannot exit these sites. Time from
infection to oviposition is 65 to 90 days. Infections may persist for 20 years in humans. Animals such as pigs,
dogs, and a variety of feline species can also harbor P. westermani.
|
| |
|
Summary |
|
Organism |
Transmission |
Symptoms |
Diagnosis |
Treatment |
S.
mansoni
S. japonicum |
skin penetration by
cercaria |
Dermatitis,
abdominal pain, bloody stool, peri-portal fibrosis, hepato-splenomegaly,
ascites, CNS |
Eggs
in stool |
Praziquantel |
| Schistosoma
hematobium |
skin
penetration by cercaria |
Dermatitis,
urogenital cystitis, urethritis and bladder carcinoma |
Eggs
in urine |
Praziquantel |
| Fasciolopsis
buski |
Metacercaria
on water chestnut |
Epigastric
pain, nausea, diarrhea, edema, ascites |
Eggs
in stool |
Praziquantel, |
|
C. sinensis
O. felinus
O. viverini |
Cysts
in fish |
Inflammation
and deformation of bile duct, hepatitis, anemia and edema |
Eggs
in stool |
Praziquantel |
|
Paragonimus
westermani |
Cyst in crab meat |
Cough (dry / rusty
brown sputum), pulmonary pain, pleurisy, tuberculosis-like |
Eggs in sputum |
Praziquantel |
|
|
 Return to the Parasitology Section of Microbiology and Immunology On-line
Return to the Parasitology Section of Microbiology and Immunology On-line
This page last changed on
Sunday, February 22, 2015
Page maintained by
Richard Hunt
|

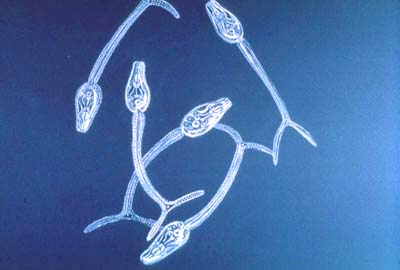 Figure 1A
Figure 1A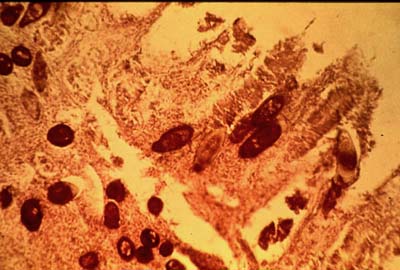 Figure 1C
Figure 1C
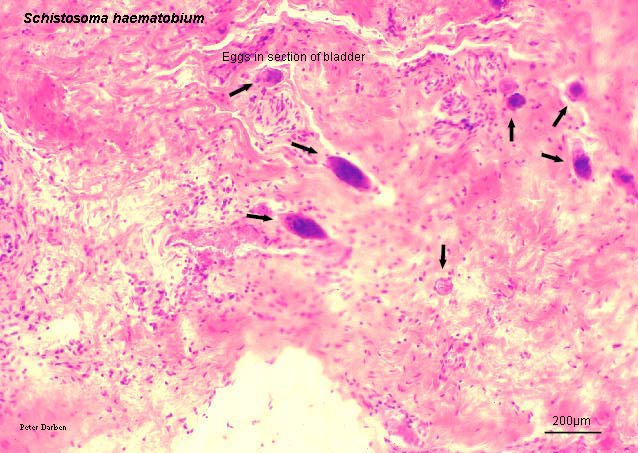 Figure 1G
Figure 1G B
B
 Figure 1K
Figure 1K Figure 1O
Figure 1O Figure 1Q
Figure 1Q Figure 1S
Figure 1S Figure 1T
Figure 1T Figure 2A
Figure 2A Figure 2C
Figure 2C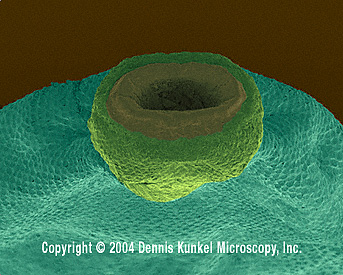 Figure 3A
Figure 3A Figure 3C
Figure 3C Figure
4
Figure
4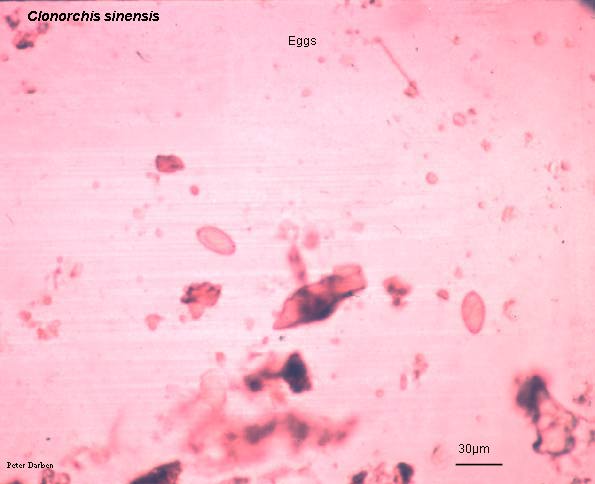 Figure 5A
Figure 5A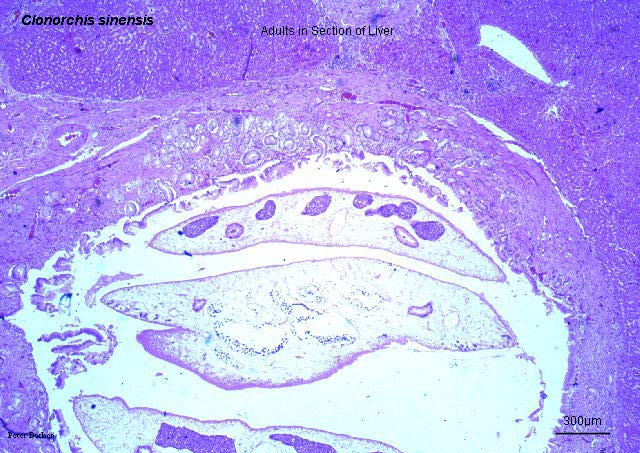 Figure 5C
Figure 5C Figure 6
Figure 6 Figure 7A
Figure 7A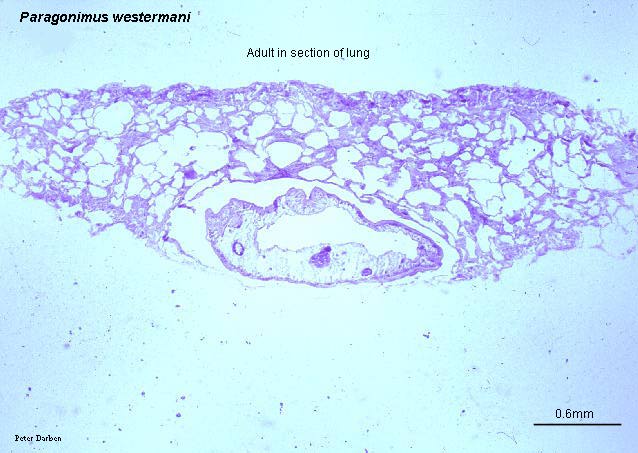 Figure 7C
Figure 7C Figure 8
Figure 8