| x | x | ||||||||||||||||||||||||||||
|
|
 |
||||||||||||||||||||||||||||
| BACTERIOLOGY | IMMUNOLOGY | MYCOLOGY | PARASITOLOGY | VIROLOGY | |||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||
|
Let us know what you think |
|||||||||||||||||||||||||||||
|
|
|||||||||||||||||||||||||||||
|
|
|||||||||||||||||||||||||||||
|
Logo image © Jeffrey Nelson, Rush University, Chicago, Illinois and The MicrobeLibrary |
|||||||||||||||||||||||||||||
|
Brief review of structure and properties of rubella virus. Discussion of viral pathogenesis and disease, epidemiology, prevention and treatment. |
Rubella virus is the only member of the Rubrivirus genus of the Togavirus family. Rubella (which means "little red" and is also known as German measles because it was first described in Germany) was originally though to be a variant of measles. It is a mild disease and often goes unnoticed in children and adults, but can cause devastating problems if it infects the fetus, especially if infection occurs during the first few weeks of pregnancy.
|
||||||||||||||||||||||||||||
 Figure
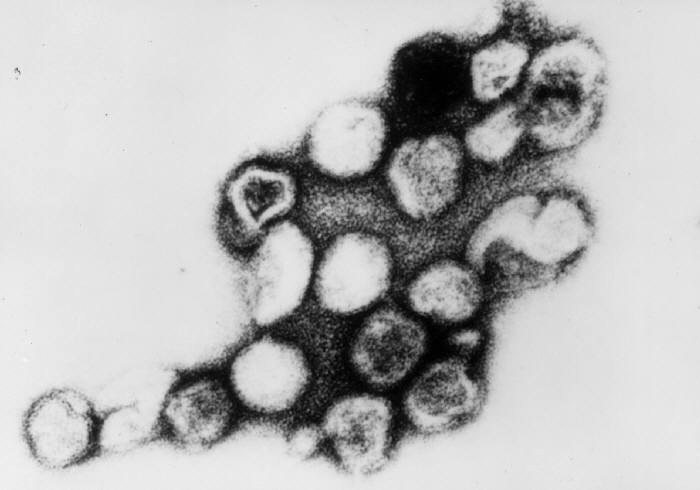
1 Electron micrograph of rubella virus CDC/Dr. Erskine Palmer Figure
1 Electron micrograph of rubella virus CDC/Dr. Erskine Palmer |
THE VIRUS Rubella virus (figure 1) is the only
member of the Rubivirus genus of the Togavirus family.
Unlike most Togaviruses it is NOT arthropod-borne, but is acquired via
the respiratory route.
It is an enveloped (toga=cloak), non-segmented, positive sense, RNA virus and
replicates in
the cytoplasm.
Its nucleocapsid has icosahedral symmetry (figure 2).
|
||||||||||||||||||||||||||||
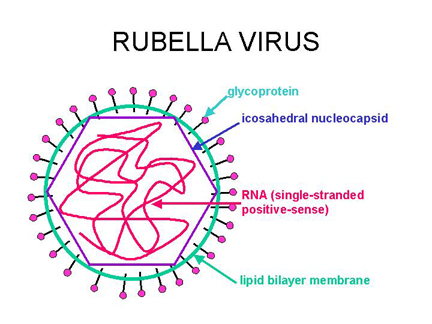 Figure 2 Structure of rubella virus
Figure 2 Structure of rubella virus
|
PATHOGENESIS AND DISEASE
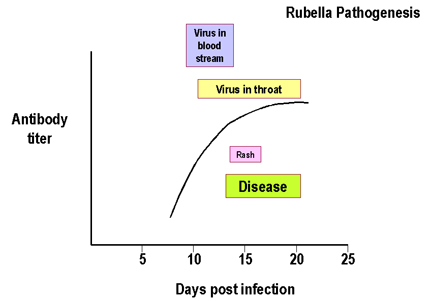
CHILDREN AND ADULTS Man is the only host. Rubella virus is spread via an aerosol route and occurs throughout most of the world although endemic rubella, like measles, has been eliminated in North America. The initial site of infection is the upper respiratory tract. The virus replicates locally (in the epithelium, lymph nodes) leading to viremia and spread to other tissues. As a result the disease symptoms develop. Rash. if it occurs, (table 1) starts after an incubation period of approximately 2 weeks (12 to 23 days) from the initial infection. There is probably an immunological basis for the rash (since it occurs as antibody titers rise). The patient is infectious from about 1 week before onset of rash to about 1 week after (figure 3). There is usually no prodrome in young children but in older children and adults disease results in
In about half of all rubella infections there are no noticeable symptoms.
T-cell immunity plays an important role in recovery. IgM may persist for up to a year. There are also IgG, IgA responses. Complications Other rare complications include orchitis, neuritis and panencephalitis.
|
||||||||||||||||||||||||||||
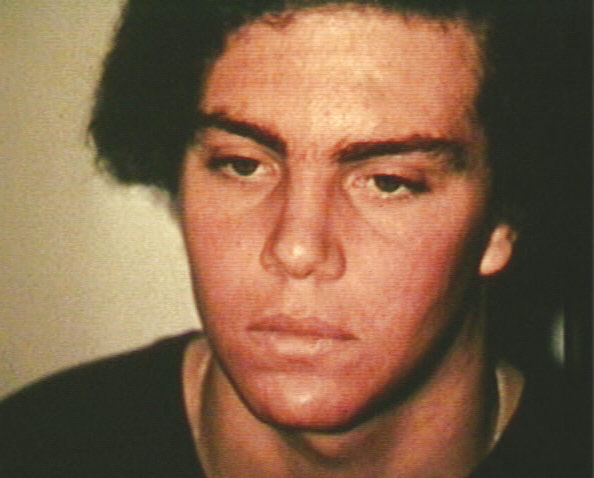
 Rubella complications CDC
Rubella complications CDC |
|||||||||||||||||||||||||||||
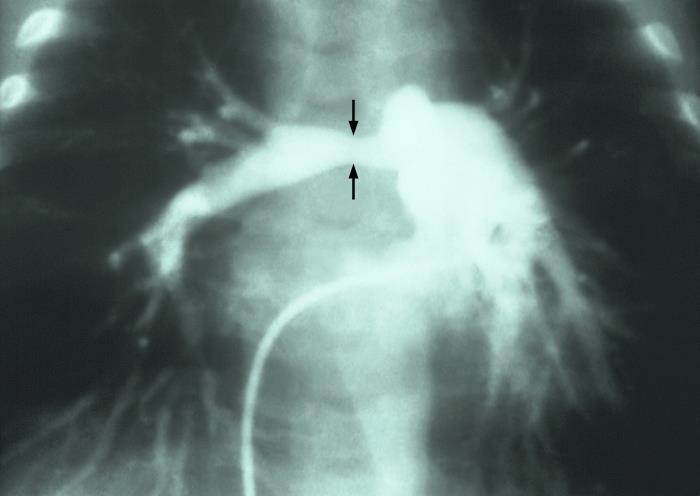 Angiocardiogram showing the pulmonary arterial tree. There is a region of constriction, also called stenosis, of the right pulmonary artery, which was due to a case of congenital rubella. CDC
|
FETUS The risk to a fetus is highest in the first few weeks of pregnancy and then declines in terms of both frequency and severity, although there is still some risk in second trimester. The virus infects the placenta and then spreads to the fetus. In an outbreak of rubella in the United States in the mid 1960's, there were over 12 million cases of rubella and 20,000 cases of congenital rubella syndrome. If non-immune mothers are infected in the first trimester, up to 80% of neonates may have devastating sequelae. However, as the result of an excellent vaccine, there have been no cases of congenital rubella syndrome in the United States in recent years.
There may also be variety of other problems including bone lesions, pneumonitis etc. In most cases, there is neural involvement - lethargy, irritability, motor tone problems, mental retardation, motor disabilities, abnormal posture, neurosensory hearing loss. Virus from congenital infections persists after birth. Those with congenital infections can infect others after birth for a year or more. Virus occurs in naso-pharyngeal secretions, urine and feces. Later on, patients with congenital rubella syndrome may develop additional complications including diabetes mellitus (up to 20%), thyroid dysfunction, growth hormone deficiency, ocular complications. Progressive rubella panencephalitis This is an extremely rare slow virus disease. It usually develops in the teens with death within 8 years. Most often it is associated with congenital rubella and may be associated with childhood rubella.
DIAGNOSIS OF RUBELLA Many (possibly 50%) infections are apparently subclinical and many infections go unrecognized, even if symptoms develop (rash is not always present). Infections with many other agents give similar symptoms to rubella (e.g. infection with human parvovirus, certain arboviruses, many of the enterovirus group of picornaviruses, some adenoviruses, Epstein-Barr virus, scarlet fever, toxic drug reactions). Serological tests, RT-PCR or
isolation of virus (immunofluorescence) are needed to confirm infection of individual. Man is the only host and rubella occurs in many countries of the world. Periodic epidemics occur in an unvaccinated population; however, natural infection protects for life because there is a single serotype.
PREVENTION A live vaccine (attenuated strain) is available. The vaccine virus is grown in human diploid fibroblasts. Since there is only one serotype, a univalent attenuated vaccine can provide lifelong immunity. The vaccine strain does not spread to family members. Normally it is given as part of a trivalent inoculation (mumps, measles and rubella vaccine). It is important that women are vaccinated prior to their first pregnancy. United States recommendations are for childhood vaccination to prevent epidemics, combined with vaccination of susceptible, non-pregnant adolescent and adult females. The vaccine is contraindicated for pregnant women, but when unwittingly used, no problems have been seen. If the patient is pregnant and seronegative, the pregnancy should be monitored carefully and the patient vaccinated postpartum. To maintain elimination of rubella, it is important that all children receive the vaccine unless there are specific contraindications.
TREATMENT There is no specific treatment. Supportive care should be used.
|
||||||||||||||||||||||||||||
|
|
|||||||||||||||||||||||||||||





{kind=link}