|
x |
x |
|
 |
 |
|
INFECTIOUS
DISEASE |
BACTERIOLOGY |
IMMUNOLOGY |
MYCOLOGY |
PARASITOLOGY |
VIROLOGY |
|
TURKISH |
BACTERIOLOGY - CHAPTER TWELVE
Streptococci
GROUPS A, B, d AND OTHERS
enterococcus faecalis
Dr Alvin Fox
Emeritus Professor
University of South Carolina School of Medicine
|
|
SLOVAK |
|
SPANISH |
|
ALBANIAN |
|
|
|
SEARCH |
Let us know what you think
FEEDBACK |
|
|

 |
|
Logo image © Jeffrey
Nelson, Rush University, Chicago, Illinois and
The MicrobeLibrary |
|
|
|
KEY WORDS
Lancefield groups
Hemolysis (alpha, beta,
gamma)
Group A streptococcus (S. pyogenes)
Bacitracin susceptibility test
M, T, R proteins
Streptolysins O and S
Lipoteichoic acid
Rheumatic fever/carditis/arthritis
Glomerulonephritis
Scarlet fever
Toxic shock-like syndrome/bacteremia
"Flesh-eating bacteria"
Erythrogenic (Pyrogenic) toxin
Group B streptococcus (S.agalactiae)
Neonatal septicemia/meningitis
CAMP test
Hippurate hydrolysis test
Group D streptococcus
Urinary tract infection/ Endocarditis
Bile-esculin test
Enterococci
Non-enterococci
Group C, G, F (large colony)
S. anginosus (minute colony)
Viridans streptococci
Dental caries/endocarditis
|
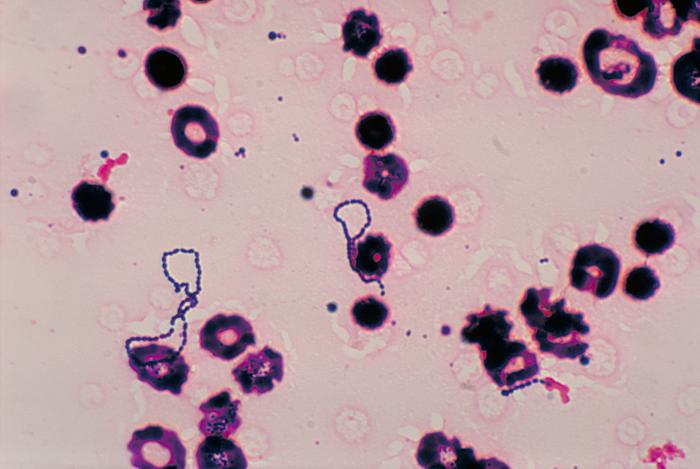
Streptococci are facultatively anaerobic, Gram-positive organisms that often
occur as chains or pairs (figures 1 and 2) and are
catalase-negative (in
contrast, staphylococci are catalase
positive) (figure 3). Streptococci are subdivided into groups by antibodies that
recognize surface antigens (figure 4). These groups may include one or more species. The
most important groupable streptococci are A, B and D. Among the groupable
streptococci, infectious disease (particularly pharyngitis) is caused by group A
which is thus emphasized here. Streptococcus pneumoniae (a major cause of
human pneumonia) and Streptococcus mutans and other so-called viridans
streptococci (among the causes of dental caries) do not possess group antigens.
Three types of hemolysis reaction (alpha, beta,
gamma) are seen after growth of streptococci on
sheep blood agar. Alpha refers to partial hemolysis with a
green coloration (from production of an unidentified product of hemoglobin) seen
around the colonies; beta refers to complete clearing (figure 5) and gamma means there
is no lysis. Group A and group B streptococci are beta hemolytic, whilst D are
usually alpha or gamma. Streptococcus pneumoniae and viridans
("green") streptococci are alpha hemolytic. Thus, the hemolysis
reaction is important in grouping streptococci. The hemolysis reaction along
with one physiologic characteristic is sufficient for a presumptive clinical
identification.
Group A streptococcus (S. pyogenes)
Most group A streptococcal infections are relatively mild illnesses but
sometimes infection by these bacteria can result in severe and life-threatening
diseases. There are several million cases of strep throat and impetigo each
year.
Streptococcus pyrogenes frequently causes
suppurative, but non-invasive
pharyngitis
(Strep Throat)
(figure 6),
and less frequently the skin infection,
impetigo. In the middle part of the
1900's, the serious complications of group A streptococcal infections began to decline
dramatically and had greatly decreased by the 1970's. Thus, interest in this
organism waned. In the 1980's and 1990's, there was an upsurge in classical
"rheumatic fever" (a non-suppurative disease of the heart) but also
new forms of streptococcal disease which include both "invasive" bacteremia, a toxic shock-like syndrome (as seen with Staphyllococcus aureus) and
so-called "flesh eating" bacteria.
Group A streptococcal infections affect all ages with peak incidence at 5
to15
years of age. The serious complications (including rheumatic fever and invasive bacteremia) were felt to affect primarily those with some underlying defect in
their immune system (including infants, elderly people and those
immunocompromised). However, it is clear now that previously healthy children
and adults are definitely at risk of serious complications.
Strep Throat
Strep throat is an infection in the throat and tonsils caused by group A
Streptococci. The disease is spread through contact with aerosols produced
in a cough or sneeze of an infected person. It can also be spread by
drinking or eating from a utensil used by an infected person. It is also
possible to get strep throat from contact with sores from group A strep skin
infections.
Common Symptoms of Strep Throat include (CDC):
- Sore throat, usually starting quickly
- Severe pain when swallowing
- Fever (101° F or above)
- Red and swollen tonsils, sometimes with white patches or streaks of
pus
- Tiny red spots (petechiae, figure 6) on the soft or hard palate—the
area at the back of the roof of the mouth
- Headache
- Nausea and/or vomiting
- Swollen lymph nodes in the neck
- Body aches
- Rash
Rheumatic fever
Rheumatic fever, is an inflammatory disease affecting
primarily the heart and joints. Although severe, it can take an extended period
of time to develop. The mechanism of chronic immunopathology of rheumatic fever
is not resolved. M protein cross-reacts with heart myosin leading to
autoimmunity. Also the group A streptococcal cell wall is highly resistant to
degradation in the host. These antigens persist for months in vivo and
experimentally elicit diseases that resemble rheumatic arthritis and carditis.
Rheumatic arthritis should not be confused with the most common rheumatic
disease - rheumatoid arthritis. Early termination of throat infections with
penicillin therapy decreases the incidence of the subsequent development of
rheumatic carditis.
Acute glomerulonephritis.
This is an immune complex disease of the kidney.
Scarlet fever
Scarlet fever usually begins with a fever
and sore throat which may be accompanied by:
- chills
- vomiting
- abdominal pain
- the tongue may have a whitish
coating and appear swollen. It may also
have a "strawberry"-like (red and bumpy)
appearance
- the throat and tonsils may be very
red and sore leading to pain in
swallowing
One or two days after the onset of
illness, a
characteristic red rash appears
(although the rash can appear before illness
or up to 7 days later).
The rash, which is caused by erythrogenic (pyrogenic)
toxins that are phage encoded, gives the
name: Scarlet Fever. Initially, the
rash is seen on the neck, under the arms,
and in the groin. It then spreads to other
parts of the body. First the rash appears as
flat red patches which gradually become fine
bumps and feel like sandpaper (figure 7).
The cheeks may have a flushed appearance but
sometimes there is a pale area around the
mouth. Underarm, elbow and groin skin
creases may become brighter red than the
rest of the rash (Pastia's lines). The rash
generally subsides in about a week and the
skin may peel around the finger tips, toes,
and groin area. This can last up to several
weeks.
Treatment is by antibiotics.
Bacteremia, toxic-shock syndrome and
necrotizing fasciitis
Normally, infection by group A Streptococci
results in mild symptoms. However, these bacteria can also cause a
bacteremia resulting in a much more severe disease which can sometimes be
fatal. Such diseases include:
- A toxic shock-like disease (including rash,
fever and shifting of fluid from the bloodstream to peripheral tissues with
resulting edema). This causes blood pressure to drop rapidly and organs (e.g.,
kidney, liver, lungs) to fail.
- and/or necrotizing
myositis and
fasciitis.
Necrotizing fasciitis (which has earned Group A Streptococci the name
"the flesh-eating bacteria") rapidly destroys muscles, fat, and skin
tissue.
Production of pyrogenic toxins (A, B and C) are a hallmark of these strains.
Pyrogenic toxin
is a superantigen (a mitogen) for T cells causing non-specific activation of the
immune system. This may be involved in the pathogenesis. This disease is still
uncommon but can progress very quickly (a few days) and is life-threatening.
Approximately 9,000 to 11,500
cases of invasive Group A Streptococcal disease
occur each year in the United States and lead to
1,000 to 1,800 deaths annually. Thus death
occurs in 10%-15% of all invasive cases,
approximately 40% of patients with streptococcal
toxic shock syndrome and approximately 25% of
necrotizing fasciitis cases die from the infection.
CDC list the
early signs and symptoms
of necrotizing
fasciitis. These
include:
- Severe pain and
swelling, often
rapidly increasing
- Fever
- Redness at a
wound site
Early signs and
symptoms of toxic shock
syndrome include:
- Sudden onset of
generalized or
localized severe
pain, often in an
arm or leg
- Dizziness
- Flu-like
symptoms such as
fever, chills,
muscle aches,
nausea, vomiting
- Confusion
- A flat red rash
over large areas of
the body (only
occurs in 1 in 10
cases)
High dose penicillin and clindamycin are used for treatment of necrotizing fasciitis and toxic shock syndrome along with supportive care in an intensive care unit in very severe cases. Early and aggressive surgery, which may reduce the fatality rate, is often needed to remove damaged tissue and stop disease spread.
|
 Figure 1
Figure 1
Streptococcus mutans. Gram stain.
CDC/Dr. Richard Facklam
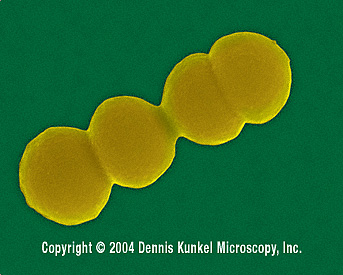
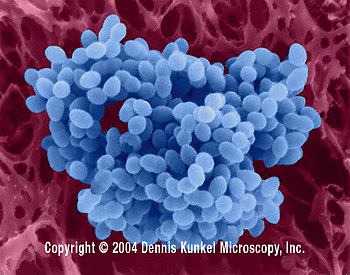
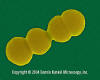 Figure 2
Figure 2
Streptococcus pyogenes - coccoid prokaryote (dividing); causes
pharyngitis, sinusitis, otitis media (middle ear infection), food poisoning, puerperal fever (childbed fever), skin and wound infections (scarlet fever, erysipelas, impetigo) . Group A
strep.
SEM x56,000 ©
Dennis Kunkel Microscopy, Inc.
Used with permission |
General features in pathogenesis
The identity of the
adhesin allowing adhesion to the respiratory epithelium
(via
fibronectin) is somewhat controversial. Lipoteichoic acid is localized in
the cell membrane of many bacteria. For group A streptococci, much is also
present in the
fimbriae on the cell exterior. Classical work suggests
lipoteichoic acid is the group A streptococcal adhesin although more recently a
role for an "F (fibronectin-binding) protein" has been suggested.
Group A streptococci in the absence of fibrinogen fix
complement to the
peptidoglycan layer and, in the absence of antibodies, are not phagocytosed. The M
protein (also found in fimbriae) binds fibrinogen from serum and blocks the
binding of complement to the underlying peptidoglycan. This allows survival of
the organism by inhibiting phagocytosis. However, in immune individuals,
neutralizing antibodies reactive with M protein elicit phagocytosis which
results in killing of the organism. This is the major mechanism by which
immunity is able to terminate group A streptococcal infections. M protein
vaccines are thus a major candidate for use against rheumatic fever. The capsule
of group A streptococci classically was stated to have limited anti-phagocytic
activity. Many of the newly described virulent strains are highly mucoid and the
capsules are important in pathogenesis.
Unfortunately, certain M protein types cross-react antigenically with the
heart and may be responsible for rheumatic carditis. The fear of autoimmunity
has rightly inhibited the use of group A streptococcal vaccines. However,
distinct protective versus cross-reactive epitopes have been defined and the
availability of a vaccine appears likely. M proteins vary antigenically between
strains; thus immunity to one M protein does not imply general immunity to all S.
pyogenes strains. M typing along with other antigens (T and R) are used for
serotyping.
|

 Figure 3
Figure 3
Catalase positive and negative test. In this test, hydrogen peroxide is
converted to oxygen (seen as gas bubbles) ©
Karen M.
Kiser. St Louis Community College, Clinical Laboratory, St.
Louis, MO
MOVIE
Catalase test
© The
MicrobeLibrary and Neal R. Chamberlain, Department of Microbiology,
Kirksville College of Osteopathic Medicine, Kirksville, Missouri |
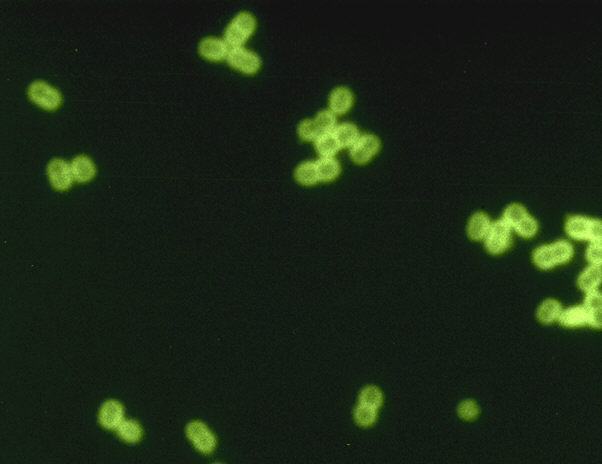
 Figure 4
Figure 4
Streptococcus fluorescent antibody stain (digitally colorized). Six
groups are in this genus: A, B, C, D, F, and G, which and are often found in
pairs or chains
CDC/Dr. M.S. Mitchell
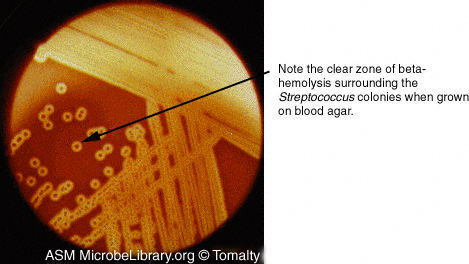
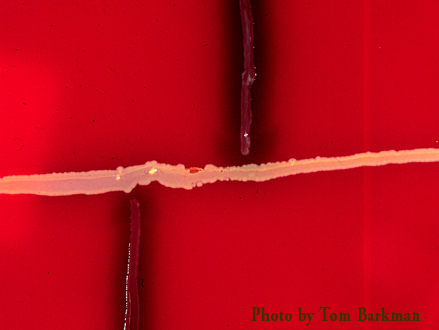
 Figure 5
Figure 5
Streptococcus pyogenes on a blood agar plate. These organisms
produce a variety of toxins, some of which are capable of lysing or destroying
erythrocytes). The result is a clear zone surrounding the bacterial colonies.
This complete destruction of the erythrocytes in the agar medium is termed beta-hemolysis.
©
The
MicrobeLibrary and Gloria J. Delisle, Queens University
Kingston, Ontario, Canada
 Figure 6
Figure 6
Strep throat is caused by group A Streptococcus bacteria. These bacteria
are spread through direct contact with mucus from the nose or throat of persons
who are infected, or through contact with infected wounds or sores on the skin.
Note the inflammation of the oropharynx and petechiae, or small red spots on the
soft palate caused by Strep Throat. CDC/Dr.
Heinz F. Eichenwald
 Figure 7
Figure 7
Skin lesions on the chest of a woman with scarlet fever. The rash first appears
as tiny red bumps on the chest and abdomen, then spreads all over the body. It
resembles a sun burn, and feels like a rough piece of sandpaper. It is usually
redder in the axillary and groin areas. CDC
|
|
|
Laboratory diagnosis
1. Direct detection - the antigen is extracted from a throat swab. The
antigen extract will then bind with antibody specific to the group A
streptococcal carbohydrate. This has classically involved agglutination of
antibody coated beads. However, simpler tests have been recently introduced. Results are available within
minutes.
2.
Lancefield grouping of isolated beta hemolytic colonies (see above).
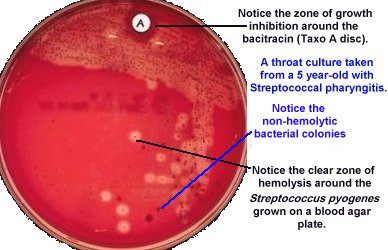
3. Colonies are beta hemolytic (figure 5) and their growth is inhibited by bacitracin
(presumptive diagnosis) (figure 7a).
4. Patient serum shows antibodies to streptolysin O or other streptococcal
antigens. This is important if delayed clinical sequelae occur.
Beta hemolysis is caused by two hemolysins O and S; the former is inactive
in the presence of oxygen. Thus, stabbing of the plate increases the intensity of
the hemolysis reaction.
|
 Figure 7a
Figure 7a
One way to differentiate beta-hemolytic group A
Streptococcus from other beta-hemolytic streptococci is by determination
of their sensitivity to bacitracin. Streptococcus pyogenes (group
A beta-hemolytic) is sensitive to bacitracin and will not grow around
the antibiotic- containing disc. The other beta-hemolytic streptococci
are not sensitive to bacitracin and will grow next to the
antibiotic-containing disc.
©
The
MicrobeLibrary
and Neal R. Chamberlain, Department of Microbiology,
Kirksville College of Osteopathic Medicine, Kirksville, Missouri
|
| |
Group B streptococcus
Streptococcus agalactiae
Group B Streptococci, which are common in the alimentary tract, cause illness
in people of all ages. In adults, group B streptococci most commonly cause
invasive bloodstream infections (bacteremia), pneumonia, skin and soft-tissue
infections, and bone and joint infections.
In newborns, these bacteria can cause
sepsis
(septicemia), pneumonia and sometimes neonatal
meningitis.
The neonatal meningitis and septicemia occur after transmission
from the normal vaginal flora of the mother. Antibiotics given during
labor can be very effective at preventing transmission.
According to CDC, about 19,800 cases occur each year in the United States in
all age groups; approximately 7,600 cases occurred in newborns before recent
prevention strategies. The rate of early-onset infection decreased from 1.7
cases per 1,000 live births in 1993 to 0.28 cases per 1,000 live births in 2008.
Since active prevention began in the mid 1990s, the rate of group B strep
disease among newborns in the first week of life has declined by 80%. The
incidence among blacks approximately twice that of non-blacks for all age
groups.
Adult infections
The rate of invasive disease is about 7 cases per 100,000 non-pregnant
adults and increases with age with an average age in non-pregnant adults of
about 60 years. The rate is highest among adults 65 years and older (20 to
25 cases per 100,000). Most adult group B disease occurs in adults with
other medical conditions including:
- diabetes mellitus
- cardiovascular disease
- congestive heart failure
- cancer
- obesity
Serious group B strep infections in adults can be fatal. On average, 8%
of adults with invasive group B strep infections (infections where the
bacteria have entered a part of the body that is normally not exposed to
bacteria) die. Risk of death is lower among younger adults, and adults who
do not have other medical conditions.
The most common problems caused by group B streptococci in adults are:
- Bloodstream infections
- Pneumonia
- Skin and soft-tissue infections
- Bone and joint infections
Group B streptococci can also lead to rare cases of meningitis.
The cause of adult infections is unknown but it may be from fecal
contamination. Diagnosis is as used with newborns and treatment is with
antibiotics (penicillin). On some occasions, infections of bone and soft
tissue require surgery.
Newborns
Most newborns with early-onset disease (less than 7 days old) have
symptoms on the day of birth. Babies who develop late-onset disease (7 to 90
days old) may appear healthy at birth and develop symptoms of group B strep
disease after the first week of life.
Symptoms include (CDC):
- Fever
- Difficulty feeding
- Irritability, or lethargy (limpness or hard to wake up the baby)
- Difficulty breathing
- Blueish color to skin
Late-onset disease sometimes also results from mother to baby
transmission, but sometimes the bacteria come from another source. For a
baby whose mother does not test positive for group B strep, the source of
infection for late-onset disease is often unknown. The fatality rate in
newborns is about 5%.
Diagnosis
The disease is diagnosed when the
bacteria are grown from samples of
the infants blood or spinal fluid.
The organism can be identified on the basis of beta hemolysis, hydrolysis
of hippurate and the CAMP reaction (figure 8). CAMP is an abbreviation for the names of the
four individuals who originally described the test. Group B streptococci produce a
factor that increases beta hemolysis of an S. aureus indicator strain.
Risk
Factors
Some pregnant women are at higher
risk of having a baby with
early-onset disease. Risk factors
include (CDC):
- Testing positive for group B
strep late in the current
pregnancy (35 to 37 weeks
gestation)
- Detecting group B strep in
urine during the current
pregnancy
- Delivering early (before 37
weeks gestation)
- Developing fever during
labor
- Having a long period between
water breaking and delivering
- Having a previous infant
with early-onset disease
Late-onset disease is more common
among premature babies (less than 37
weeks). Babies with group B strep
positive mothers also have a higher
risk of late onset disease.
|
|
|
|
|
 Figure 8a
Figure 8a
CAMP positive reaction
©
Karen
M. Kiser. St Louis Community College, Clinical Laboratory,
St. Louis, MO
 Figure 8b
Figure 8b
CAMP negative reaction
©
Karen
M. Kiser. St Louis Community College, Clinical Laboratory,
St. Louis, MO


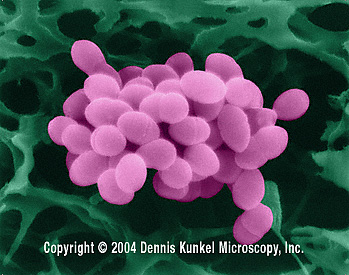
Figure 9
Streptococcus faecalis - coccoid prokaryote (dividing); a pathogen causing skin and wound infections ©
Dennis Kunkel Microscopy, Inc.
Used with permission


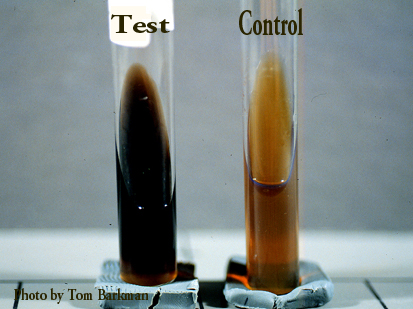
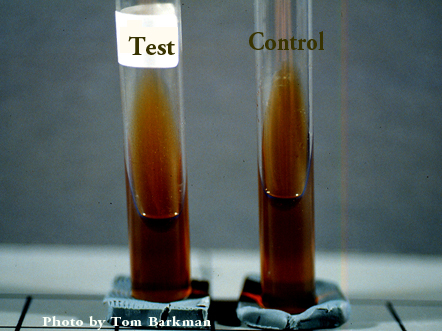
Figure 10
Bile esculin test. Group D streptococci are positive in this test (Above:
Positive. Below: Negative)
©
Karen
M. Kiser. St Louis Community College, Clinical Laboratory,
St. Louis, MO

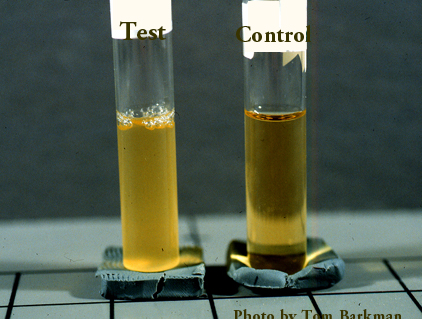
 Figure 11
Figure 11
Positive growth in 6.5% sodium chloride (top) and no growth in a similar medium
(bottom)
©
Karen
M. Kiser. St Louis Community College, Clinical Laboratory,
St. Louis, MO
|
|
 Figure 12
Figure 12
The bacterium Streptococcus viridans, is responsible for
approximately half of all cases of bacterial endocarditis, but is found
in the mouth as normal oral bacterial flora. CDC/Dr.
Mike Miller
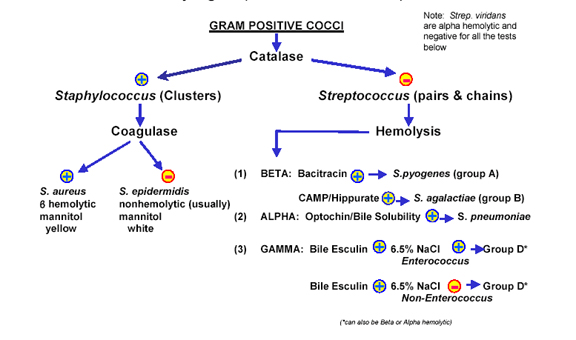
 Streptococccus identification scheme
Streptococccus identification scheme |
ENTEROCOCCUS
Group D streptococcus
Now classified as an
Enterococcus. The most common is E. faecalis
Enterococci are distantly related to other streptococci and have been moved into
the genus Enterococcus; the most commonly isolated is E. (S.) faecalis
(figure 9).
As the name implies enterococci are found in the gut flora where they are
usually harmless
commensals and infection often
follows from fecal contamination. They are a significant cause of urinary tract
infections (but much less common than E. coli) and also of opportunistic
infections (including intra-abdominal, septicemia and endocarditis). There are a
number of virulence factors that may contribute to E. faecalis
infections.
- A plasmid-encoded hemolysin (cytolysin)
- A plasmid-encoded factor (aggregation substance)
The cytolysin in combination with high-level gentamicin resistance is
associated with a five-fold increase in risk of death in human bacteremia
patients.
E. faecalis can cause serious human nosocomial infections in humans. This
is because the organisms shows high levels of antibiotic resistance. It is often
found in teeth after root canal operations with a prevalence from 30% to 90% of
the cases. It is resistant to many common antibiotics such as aminoglycosides,
aztreonam, cephalosporins, clindamycin, the semisynthetic penicillins nafcillin
and oxacillin, and trimethoprim-sulfamethoxazole. Resistance to vancomycin is
becoming more common.
When the bacteria are vancomycin-resistant, the patient with a urinary tract
infection may be treated with nitrofurantoin. Other options include ampicillin,
linezolid and daptomycin. In root canal treatments sodium hypochlorite and
chlorhexidine are used before isolating the canal.
Colonies are usually alpha or gamma hemolytic. Growth on bile-esculin produces a black precipitate derived from
esculin (figure 10);
many other bacteria will not grow in the presence of bile. Group D streptococci
are divided into those that will grow in 6.5% saline (enterococci) and those
that will not (non-enterococci) (figure 11).
Other beta hemolytic groups
Groups C and G (and rarely group F) occasionally cause human disease
(particularly pharyngitis).
Group C streptococci includes:
- Streptococcus equi, which causes a disease in horses
- S. zooepidemicus which causes infections in cattle and horses
among other animals
- S. dysgalactiae
Group G streptococci includes
- S. canis. This is normally found in a number of animals but can
also cause infection in humans.
Group H streptococci cause infections in dogs and rarely cause illness in
humans unless the person has direct contact with the mouth of an infected dog.
This can occur by "kissing" a dog or from saliva after being licked by an
infected dog.
Minute colony streptococci
The normal human flora contains organisms that may be group A, C, F or G or
are non-groupable (Streptococcus anginosus, Streptococcus milleri). Their role in human
disease is unclear but Streptococcus anginosus can cause diseases
including brain and liver abscesses under certain circumstances, particularly in
immuno-deficient individuals.
Viridans streptococci
These are a diverse group of commensal species commonly found orally (including S. mutans)
and cause endocarditis after release into the bloodstream from tooth
extraction (figure 12).
S. mutans is responsible for approximately half of all cases of bacterial
endocarditis. They can synthesize dextrans from glucose. This allows them
to adhere to fibrin-platelet aggregates at damaged heart valves. Thus, they have
the ability to cause sub-acute valvular heart disease following their
introduction into the bloodstream (such as by tooth extraction).
These bacteria are also involved in dental caries
and pericoronitis, an inflammation of the soft tissues surrounding the crown of
a partially erupted tooth.
They are either alpha or non- hemolytic and negative for
other tests described above. They produce a green color on blood agar plates (Viridis,
Latin: Green). Viridans streptococci can be differentiated from S. pneumoniae
using an optochin test. Viridans streptococci are optochin-resistant.
They are non-groupable.
|
|
|

Return to the Bacteriology
Section
of Microbiology and Immunology On-line
This page last changed on
Wednesday, March 02, 2016
Page maintained by
Richard Hunt
|