|
KEYWORDS
S. pneumoniae
Diplococcus
Pneumococcus
Autolysin
Bile solubility test
Optochin susceptibility
Capsule
Quellung reaction
Staphylococcus
aureus
Staphylococcus epidermidis
Coagulase positive or Coagulase negative
Alpha,
beta, gamma and delta
cytotoxins
Leucocidin
Lipase
Exfoliatin
Enterotoxins
Toxic shock syndrome
Toxic shock toxin
Protein A
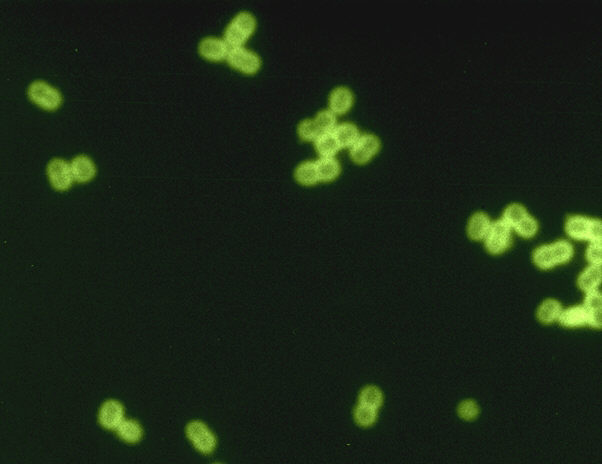
 Figure 1a Streptococcus pneumoniae in spinal fluid. FA stain (digitally colorized).
CDC/Dr. M.S. Mitchell
Figure 1a Streptococcus pneumoniae in spinal fluid. FA stain (digitally colorized).
CDC/Dr. M.S. Mitchell
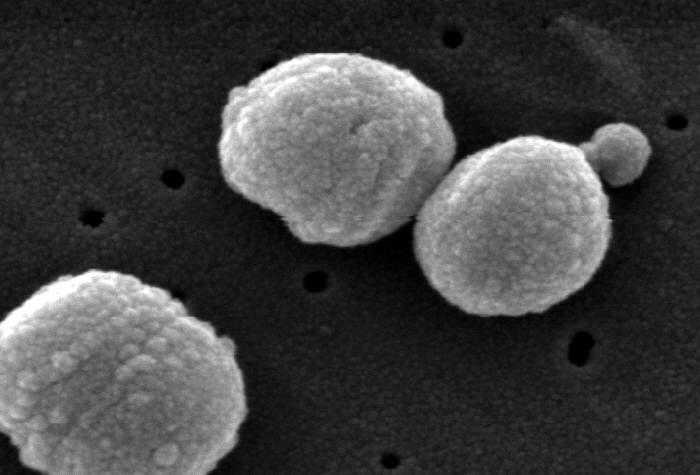
 Figure 1B Scanning Electron Micrograph of
Streptococcus pneumoniae.
CDC/Dr. Richard Facklam
rrf2@cdc.gov
Figure 1B Scanning Electron Micrograph of
Streptococcus pneumoniae.
CDC/Dr. Richard Facklam
rrf2@cdc.gov
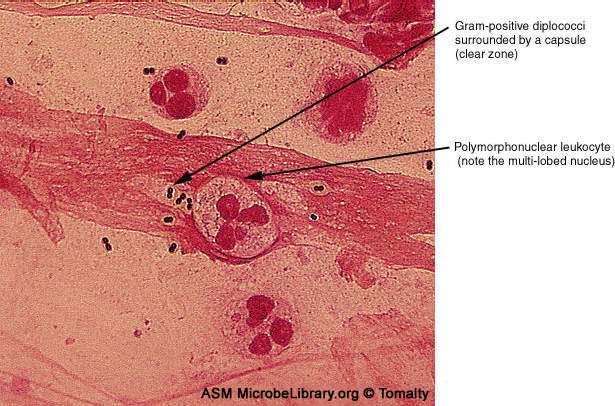
 Figure 1C Encapsulated Streptococcus pneumoniae © Gloria J. Delisle and Lewis Tomalty, Queens University, Kingston,
Ontario and
The MicrobeLibrary
Figure 1C Encapsulated Streptococcus pneumoniae © Gloria J. Delisle and Lewis Tomalty, Queens University, Kingston,
Ontario and
The MicrobeLibrary
A
 B
B
 Figure 2
Figure 2
It is difficult to
distinguish normal alpha streptococci found in the mouth from the pathogenic
Streptococcus pneumoniae. Both are alpha-hemolytic on blood agar and so must be distinguished using the "P" disk
(optochin).
S. pneumoniae
(A) is sensitive while S. mitis (B) is resistant
©
Pat Johnson, Palm Beach Community College, Lake Worth Florida
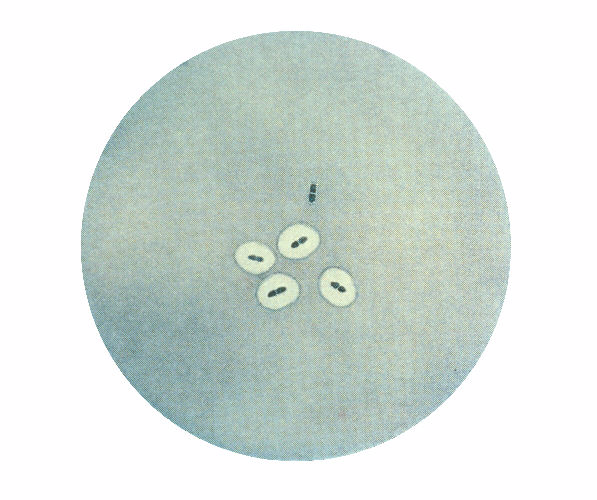
 Figure 3
Figure 3
Photomicrograph of Streptococcus pneumoniae bacteria revealing capsular
swelling using the Neufeld-Quellung test. CDC
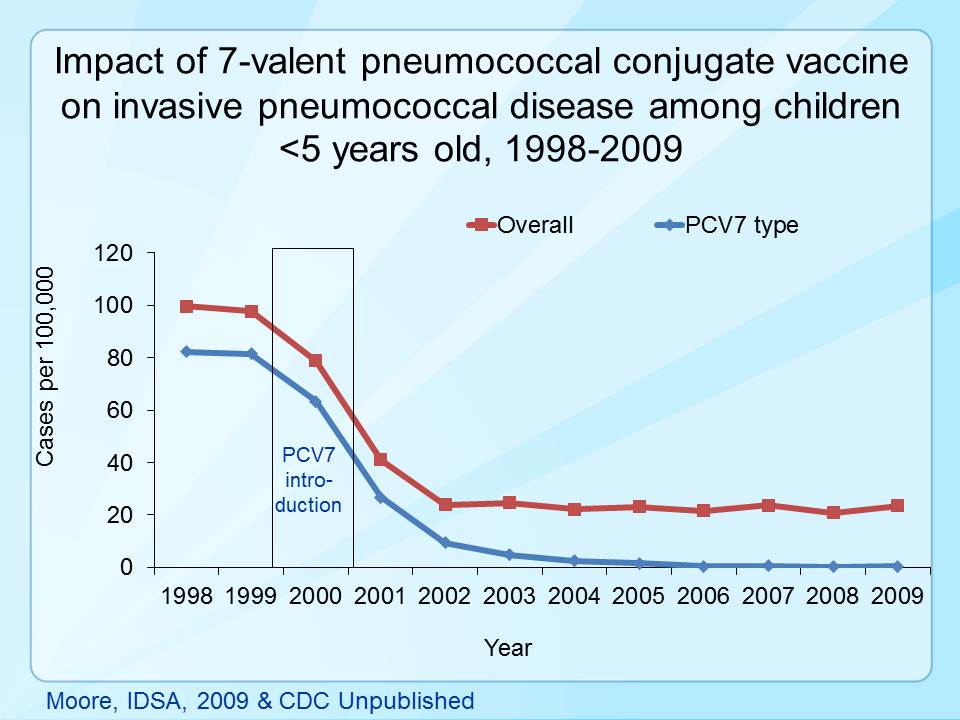
 Figure 4
Figure 4
Impact of seven valent pneumococcal vaccine on invasive pneumococcal
disease in children under 5 years of age. CDC
|
STREPTOCOCCUS PNEUMONIAE
Pneumococcal Disease
S. pneumoniae (figure 1) is a leading cause of pneumonia in all ages (particularly the young
and old), often after "damage" to the upper respiratory tract (e.g.
following viral infection). It also causes middle ear infections (otitis media).
The organism often spreads causing bacteremia and meningitis. S. pneumoniae
is α hemolytic and there is no group antigen.
Risk factors for pneumococcal disease in
children (CDC)
- Younger than 2 years of age
- In group child care
- Certain illnesses (sickle cell disease, HIV infection, and
chronic heart or lung conditions)
- Cochlear implants or cerebrospinal fluid (CSF) leaks (escape
of the fluid that surrounds the brain and spinal cord)
Some American Indian, Alaska Native, and African American
children may also be at increased risk.
Risk factors for pneumococcal disease in
adults (CDC)
- Chronic illnesses (lung, heart, liver, or kidney disease;
asthma; diabetes; or alcoholism)
- Conditions that weaken the immune system (HIV/AIDS, cancer,
or damaged/absent spleen)
- Living in nursing homes or other long-term care facilities
- Cochlear implants or cerebrospinal fluid (CSF) leaks (escape
of the fluid that surrounds the brain and spinal cord)
- Smoking
Serotypes
There are more than 90 strains of pneumococcus bacteria. Seven
serotypes (6A, 6B, 9V, 14, 19A, 19F, and 23F) accounted for most
drug-resistant S. pneumoniae. These serotypes are covered by the
PCV7 vaccine.
Disease and Symptoms
Pneumococcal pneumonia
According to CDC, as many as 400,000 hospitalizations from
pneumococcal pneumonia occur each year in the United States.
Pneumococci account for about 30% of adult community-acquired
pneumonia.
Pneumococcal pneumonia is the most common serious form of
pneumococcal disease and can be mild to severe in all age groups.
Complications include infection of the space between pleural
membranes (empyema), inflammation of the pericardium, the sac surrounding the
heart (pericarditis), and blockage of the airway that allows air
into the lungs (endobronchial obstruction), with lung collapse (atelectasis)
and collection of pus (abscess) in the lungs.
It is fatal in about five per cent of patients with non-invasive
pneumococcal pneumonia, but the rate may be higher among elderly
patients.
Symptoms include (CDC):
- Fever and chills
- Cough
- Rapid breathing or difficulty breathing
- Chest pain
- Confusion or low alertness in older patients, rather than
the more common symptoms listed above
Pneumococcal meningitis
Pneumococcal infection causes 13 to 19% of all cases of bacterial
meningitis in the United States. An estimated 3,000 cases of
pneumococcal meningitis occur each year. This is the most severe type of invasive pneumococcal disease.
Ten per cent of children younger than 5 years old with pneumococcal
meningitis die. Those that survive may have long-term problems,
including hearing loss or developmental delay. The chance of death
increases among elderly patients.
Symptoms include (CDC):
- Stiff neck
- Fever and headache
- Pain when looking into bright lights
- Confusion
- In babies, meningitis may cause poor eating and drinking,
low alertness, and vomiting.
Pneumococcal bacteremia and sepsis
About 12,000 cases of pneumococcal bacteremia occur each year in
the United States.
Asplenic patients who develop bacteremia may deteriorate very
rapidly.
Bacteremia occurs in up to 25 to 30% of patients with
pneumococcal pneumonia. The case-fatality rate is 5 to 7% and may be
higher than 60% among elderly persons. About 4% of children with pneumococcal bacteremia die of the
infection. The death rate increases among elderly patients.
Symptoms include (CDC):
- Fever
- Chills
- Low alertness
Pneumococcal otitis media
Pneumococci commonly cause of acute otitis
media. They are found in 28 to 55% of middle ear aspirates.
By age 12 months, more than 60% of children have had at least one
episode of acute otitis media. The sinuses can also be infected. These
infections are usually mild. Some children develop repeated ear infections and may
need ear tubes. It is likely that pneumococcal ear infections
account for more than 10 million visits to doctors per year in the
United States.
Symptoms include (CDC):
- Ear pain
- Red, swollen ear drum
- Sometimes fever and sleepiness
Diagnosis
Direct Gram staining or detection of capsular antigen in sputum
can be diagnostic. The organism grows well on sheep blood agar.
Autolysin
Pneumococci are identified by solubility in bile.
An autolysin (peptidoglycan-degrading enzyme) is released by bile from the cell
membrane and binds to a choline-containing teichoic acid attached to the
peptidoglycan. The autolysin then digests the bacterial cell wall resulting in
lysis of the cell. If the cells are grown in ethanolamine instead of choline,
ethanolamine is incorporated into the teichoic acid. The autolysin then cannot
lyse the cell wall. Understanding how the autolysin works has led to the suggestion
that antibiotics (including penicillin) work together with the autolysin in
killing of pneumococci in vivo.
The organisms are also identified by susceptibility to
optochin (ethyl hydrocupreine) (figure 2)
Capsule
This is highly prominent in virulent strains
(figure 1c) and its
carbohydrate antigens vary greatly in structure among strains. The capsule is
anti-phagocytic and immunization is primarily against the capsule. Capsular
vaccines are available for susceptible individuals; immunity is serotype-specific.
Using appropriate type-specific antisera, the capsule on isolated bacteria can be
"fixed" and becomes visible microscopically (the
Quellung reaction)
which is useful in microbial identification (figure 3).
The organism also produces pneumolysin
that degrades red blood cells under anaerobic conditions (observed
as alpha hemolysis).
Complement activation by teichoic acid may explain the
attraction of large numbers of inflammatory cells to the focal site of
infection.
Transmission
S. pneumoniae is transmitted person to person by
contact with saliva and mucus.
Treatment
Most strains of S. pneumoniae are susceptible to
penicillin. However, resistance is quite common and 15% of invasive pneumococcal
isolates are resistant to penicillin in some parts of the United States.
Vaccine
Pneumococcal vaccines, of which there are several types,
are very good at preventing severe disease, hospitalization and death.
Before the vaccine, there were about 700 cases of meningitis, 13,000
blood infections, and 200 deaths from pneumococcal disease each year
among children younger than 5 years old in the United States. After
vaccination started, these numbers dropped dramatically. Before
introduction of the first vaccine, rates of invasive pneumococcal
disease among children under five were approximately 80 cases per
100,000 with 10 cases per 100,000 population being pneumococcal
meningitis (figure 4).
After the
introduction of the PCV7 vaccine, rates of disease due to the seven serotypes
in the vaccine dropped
to less than 1 case per 100,000 by 2007.
The pneumococcal conjugate vaccine
(PCV13 or Prevnar 13) provides protection against the 13 serotypes
responsible for most severe illness in children.
|