|
x |
x |
|
 |
 |
|
INFECTIOUS
DISEASE |
BACTERIOLOGY |
IMMUNOLOGY |
MYCOLOGY |
PARASITOLOGY |
VIROLOGY |
|
PORTUGUESE |
Please Note: A new expanded and updated
version of this page is now available
Please go
here
MYCOLOGY - CHAPTER FOUR
SUPERFICIAL MYCOSES
Dr Art DiSalvo
Emeritus Director, Nevada State Laboratory
Emeritus Director of Laboratories, South Carolina Department of Health
and Environmental Control
|
|
TURKISH |
|
ALBANIAN |
Let us know what you think
FEEDBACK |
|
SEARCH |
|
|
|
|

 |
|
|
|
|
| |
The superficial (cutaneous) mycoses are
usually confined to the outer layers of skin, hair, and nails, and do not invade
living tissues. The fungi are called dermatophytes. Dermatophytes, or more
properly, keratinophilic fungi, produce extracellular enzymes (keratinases)
which are capable of hydrolyzing keratin.
|
 Figure 1 Onychomycosis due to Trychophyton rubrum, right and left great toe. Tinea
unguium. CDC/Dr. Edwin P. Ewing, Jr.
Figure 1 Onychomycosis due to Trychophyton rubrum, right and left great toe. Tinea
unguium. CDC/Dr. Edwin P. Ewing, Jr.
epe1@cdc.gov
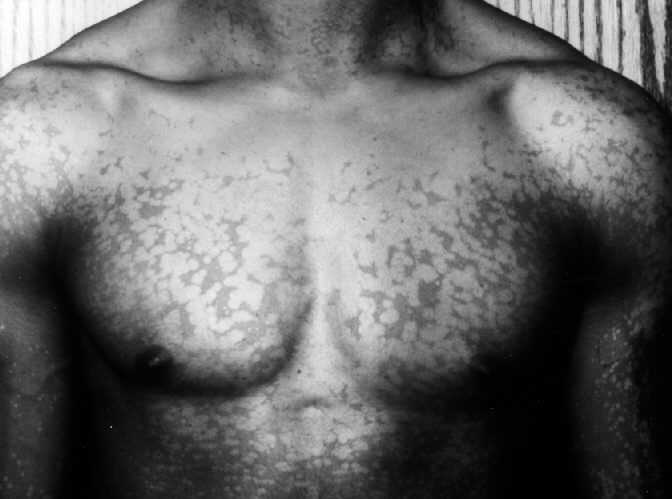
 Figure 2 Tinea Versicolor on chest.
Figure 2 Tinea Versicolor on chest.
CDC/Dr. Gavin Hart
 Figure 3.
Figure 3.
A child with a ringworm (tinea) fungal infection on the left side of his
face and left ear. “Tinea faciei” or "Tinea capitis" is the name used for infections of the
face caused by a dermatophytic fungus, but not including infection of
the bearded areas, which are called “tinea barbae”. Tinea faciei
infections are uncommon, and are often initially misdiagnosed.
CDC |
CLINICAL MANIFESTATIONS
Tinea means "ringworm" or
"moth-like". Dermatologists use the term to refer to a variety of
lesions of the skin or scalp.
Tinea corporis - small lesions occurring
anywhere on the body (figure 6, 7 and 8).
Tinea pedis - "athlete's foot". Infection of toe webs and soles of feet.
Tinea unguium (onychomycosis) - nails.
Clipped and used for culture (figure 1).
Tinea capitis - head. Frequently found
in children (figure 3 and 4).
Tinea cruris - "jock itch".
Infection of the groin, perineum or perianal area.
Tinea barbae - ringworm of the bearded
areas of the face and neck (figure 5).
Tinea versicolor - Characterized by a
blotchy discoloration of skin which may itch. Up to 25% of the general
population may have this lesion at any one time. Diagnosis is usually possible
by direct microscopic examination of KOH-treated skin scrapings which show a
typical aspect of mycelia and spores described as "spaghetti and
meatballs." Tinea versicolor is caused by Malassezia furfur (figure 2).
ECOLOGY
The dermatophytes (which means skin plants) causing
human infections may have different natural sources and modes of transmission:
anthropophilic - These are usually associated with
humans only; transmission from man to man is by close contact or through
contaminated objects.
zoophilic - These are usually associated
with animals; transmission to man is by close contact with animals (cats, dogs,
cows) or with contaminated products.
geophilic - These are usually found in the
soil and are transmitted to man by direct exposure.
Knowledge of the species of dermatophyte and source of infection are important for proper treatment of the
patient and control of the source. Invasion by zoophilic or geophilic
organisms may cause inflammatory disease in man. Geographic distribution: Dermatophytes
occur worldwide, but some species have geographically limited distribution.
|
 Figure 4
Figure 4
A child with ringworm of the scalp, called “tinea capitis”, caused by a
Microsporum sp.. Tinea capitis is an infection of the scalp caused by
mold-like fungi called dermatophytes, which thrive in warm, moist areas.
Susceptibility to tinea infection is increased by poor hygiene, prolonged
moist skin, and minor skin or scalp injuries.
CDC |
 Figure 5
Figure 5
Ringworm of the bearded areas of the face and neck, known as “tinea barbae”,
or “barber’s itch”. Tinea barbae is due to a dermatophytic infection
around the bearded area of men. Generally, the infection occurs as a
follicular inflammation, or as a cutaneous granulomatous lesion, i.e. a
chronic inflammatory reaction.
CDC
 Figure 6
Figure 6
Tinea corporis lesions, or “ringworm” on this patient’s arm due to the
dermatophytic fungus Trichophyton rubrum. Dermatophytic members of
the genus Trichophyton inhabit the soil, humans or animals, and are
some of the leading causes of hair, skin and nail infections, or
dermatophytosis in their human hosts.
CDC
 Figure 7
Figure 7
Patient with ringworm on the arm, or tinea corporis due to
Trichophyton mentagrophytes. The genus Trichophyton inhabits
the soil, humans or animals, and is one of the leading causes of hair,
skin and nail infections, or dermatophytosis in humans.
CDC/Dr. Lucille
K. Georg
 Figure 8
Figure 8
This patient, a native of New Guinea, has ringworm on the skin of the
right axilla and flank due to Trichophyton rubrum. Usually
occurring as a skin parasite, or dermatophyte on man and animals, the
genus Trichophyton is characterized by colorless spores that can
cause ringworm on the body. This condition is called Tinea corporis.
CDC/Lucille K. Georg
|
 Figure 9 Trichophyton mentagrophytes contracted from a dog
©
Bristol Biomedical Image Archive. Used with permission
Figure 9 Trichophyton mentagrophytes contracted from a dog
©
Bristol Biomedical Image Archive. Used with permission
 Figure
10 Dermatomycosis (ringworm) of hair follicles © Bristol
Biomedical Image Archive. Used with permission Figure
10 Dermatomycosis (ringworm) of hair follicles © Bristol
Biomedical Image Archive. Used with permission |
ETIOLOGIC AGENTS
There are three genera of dermatophytes:
- Trichophyton species (19 species)
(figure 9).
These infect skin, hair and nails.
They rarely cause subcutaneous infections, in immuno-compromised individuals.
Trichophyton species take 2 to 3 weeks
to grow in culture. The conidia are large (macroconidia), smooth, thin-wall,
septate (0-10 septa), and pencil-shaped; colonies are a loose aerial mycelium
that grow in a variety of colors. Identification requires special biochemical
and morphological techniques (figure 10). Trichophyton rubrum is presently the most common
cause of tinea in South Carolina. It can rarely cause sub-cutaneous infections (kerion)
in immunocompromized individuals, particularly patients with chronic myelogenous leukemia
|
| |
 Figure 10A
Figure 10A
Trichophyton conidia are large, smooth, thin-walled, septate,
and pencil-shaped
Dr Arthur DiSalvo
|
 Figure 11A Ringworm, stained preparation, macroconidia of
Microsporum canis
©
Bristol Biomedical Image Archive. Used with permission
Figure 11A Ringworm, stained preparation, macroconidia of
Microsporum canis
©
Bristol Biomedical Image Archive. Used with permission
 Figure 11B
Figure 11B
Microsporum species:
Thick wall, spindle shape, multicellular
Dr Arthur DiSalvo
 Figure 12. Microsporum canis obtained from a skin scraping of a patient with ringworm on the neck acquired from her infected cat. The fungus is identified as a dermatophyte by this calcofluor stain of the skin scrapings viewed at 500X magnification. The
calcofluor dye binds to the chitin in the fungus and fluoresces under a fluorescent light.
Figure 12. Microsporum canis obtained from a skin scraping of a patient with ringworm on the neck acquired from her infected cat. The fungus is identified as a dermatophyte by this calcofluor stain of the skin scrapings viewed at 500X magnification. The
calcofluor dye binds to the chitin in the fungus and fluoresces under a fluorescent light.
© Gloria J. Delisle, Lewis Tomalty, Queens University,
Ontario and The MicrobeLibrary
 Figure 13 Ringworm caused by Microsporum gypseum, culture plate with Sabouraud's dextrose agar
Figure 13 Ringworm caused by Microsporum gypseum, culture plate with Sabouraud's dextrose agar
© Bristol Biomedical Image Archive. Used with permission
 Figure 14
Figure 14
Epidermophyton floccosum
Dr Arthur DiSalvo |
- Microsporum species (13
species). These may infect
skin and hair, rarely nails. The prevalence of infection has decreased significantly
in recent years. When
prevalent (15-20 years ago), this organism could be easily identified on the
scalp because infected hairs fluoresce a bright green color when illuminated
with a UV-emitting Wood's light. The loose, cottony mycelia produce macroconidia
(figure 11A and B) which are thick-walled, spindle-shaped, multicellular, and echinulate (spiny).
Microsporum canis is one of the most common dermatophyte species infecting
humans.
- Epidermophyton floccosum.
These infect skin and nails and rarely hair. They form yellow-colored, cottony
cultures and are usually readily identified by the thick, bifurcated hyphae with
multiple smooth, club-shaped macroconidia (figure 14).
THERAPY
Skin infections can be treated (more or
less successfully) with a variety of drugs, such as:
Tolfnatate (Tinactin) available over the
counter - Topical
Ketoconazole seems to be most effective
for tinea versicolor and other dermatophytes.
Itraconazole - oral
Terbinifine (Lamisil) - oral,
topical.
Echinocandins (caspofungin)
For infections involving the scalp and
particularly the nails, griseofulvin is commonly used. This antimycotic must be
incorporated into the newly produced keratin layer to form a barrier against
further invasion by the fungus. This is a very slow process requiring oral
administration of the drug for long periods - up to 6 to 9 months for fingernail
infections and 12 to18 months for toenail infections.
Itraconazole and terbinafine are the drugs
of choice for onychomycoses.
THE DERMATOPHYTID REACTION
Patients infected with a
dermatophyte may show a lesion, often on the hands, from which no fungi can be
recovered or demonstrated. It is believed that these lesions, which often occur
on the dominant hand (i.e. right-handed or left-handed), are secondary to
immunological sensitization to a primary (and often unnoticed) infection located
somewhere else (e.g. feet). These secondary lesions will not respond to topical
treatment but will resolve if the primary infection is successfully treated.
|
|
|
 Return to the Mycology Section of Microbiology and Immunology On-line
Return to the Mycology Section of Microbiology and Immunology On-line
This page last changed on
Sunday, December 30, 2018
Page maintained by
Richard Hunt
|
 Figure 1 Onychomycosis due to Trychophyton rubrum, right and left great toe. Tinea
unguium. CDC/Dr. Edwin P. Ewing, Jr.
Figure 1 Onychomycosis due to Trychophyton rubrum, right and left great toe. Tinea
unguium. CDC/Dr. Edwin P. Ewing, Jr.  Figure 4
Figure 4 Figure 9 Trichophyton mentagrophytes contracted from a dog
©
Bristol Biomedical Image Archive. Used with permission
Figure 9 Trichophyton mentagrophytes contracted from a dog
©
Bristol Biomedical Image Archive. Used with permission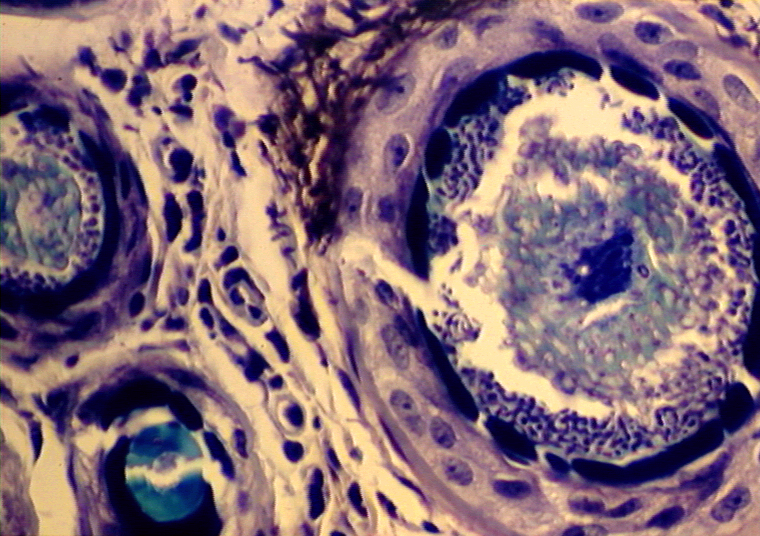 Figure
10 Dermatomycosis (ringworm) of hair follicles © Bristol
Biomedical Image Archive. Used with permission
Figure
10 Dermatomycosis (ringworm) of hair follicles © Bristol
Biomedical Image Archive. Used with permission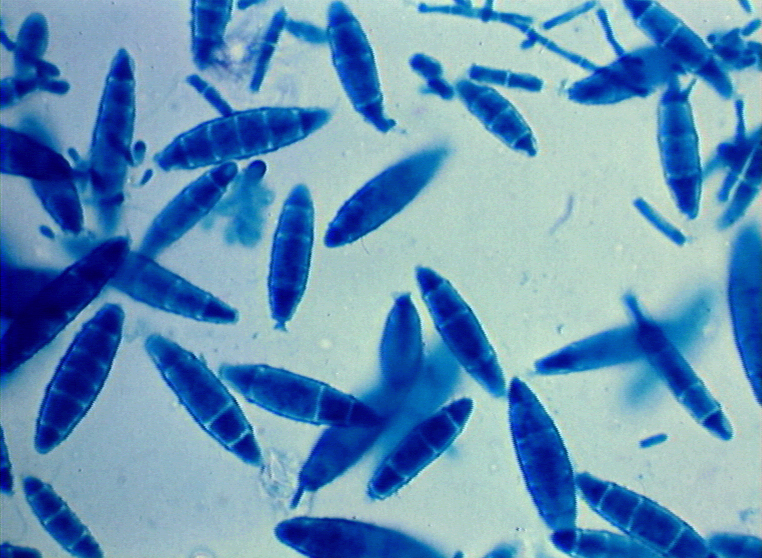 Figure 11A Ringworm, stained preparation, macroconidia of
Microsporum canis
©
Bristol Biomedical Image Archive. Used with permission
Figure 11A Ringworm, stained preparation, macroconidia of
Microsporum canis
©
Bristol Biomedical Image Archive. Used with permission